Specialized Nursing Care Procedure
Subtopic:
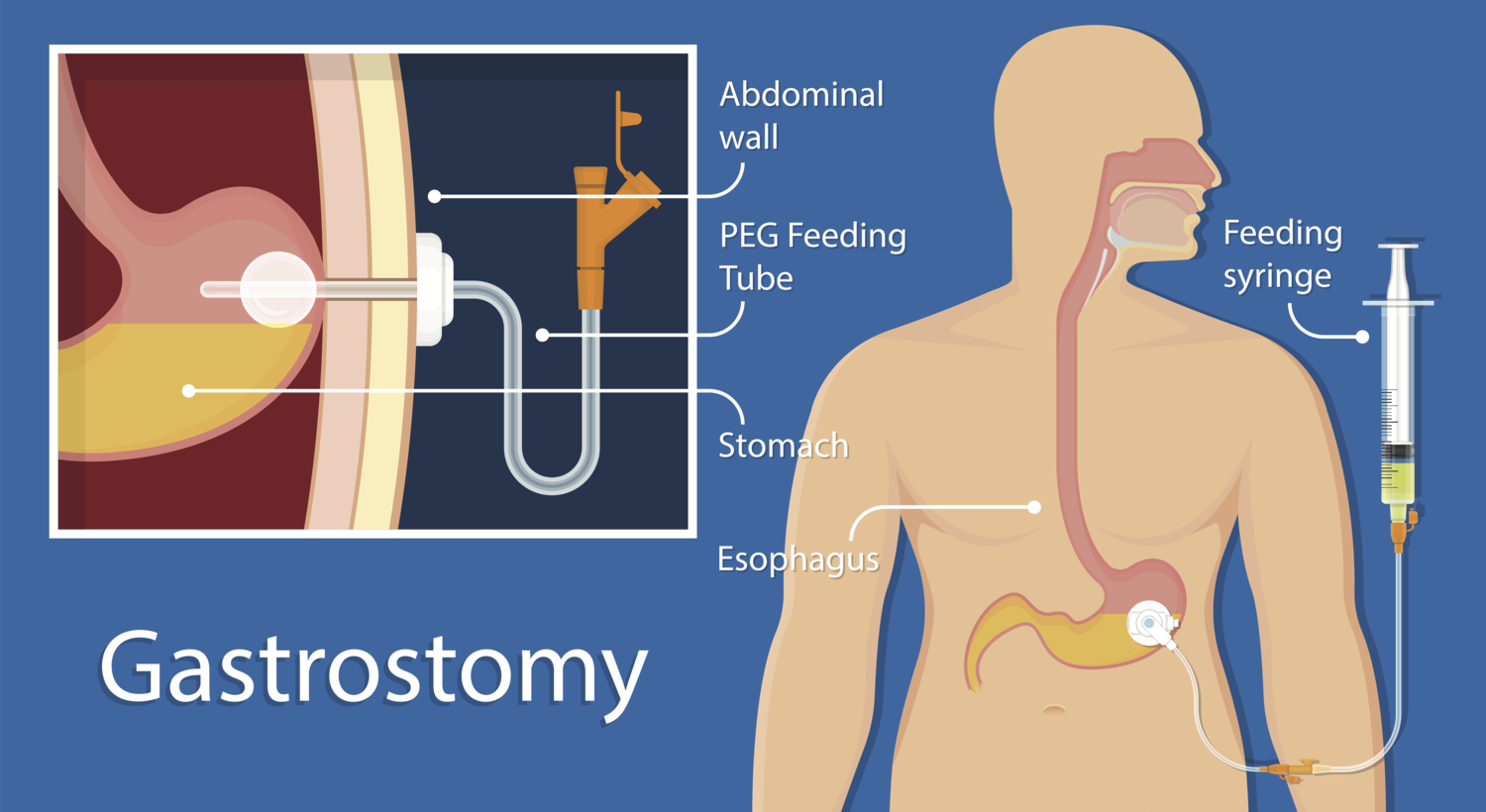
Gastrostomy feeding
Learning Objectives
Define gastrostomy feeding and describe its anatomical and clinical purpose.
Identify clinical indications for gastrostomy feeding across various patient conditions.
Differentiate types of feeding tubes and understand their placement and retention mechanisms.
Explain the procedure for administering gastrostomy feeding, including equipment setup and nursing actions.
Recognize potential complications related to gastrostomy tubes and feeding administration.
Definition-Gastrostomy feeding
Is a method of providing nutrition directly into the stomach through a surgically created opening (stoma) in the abdominal wall. A gastrostomy tube (G-tube) is inserted through this opening and held in place by an internal balloon or bumper and an external fixator. This method is used when a patient is unable to safely or adequately consume food orally.
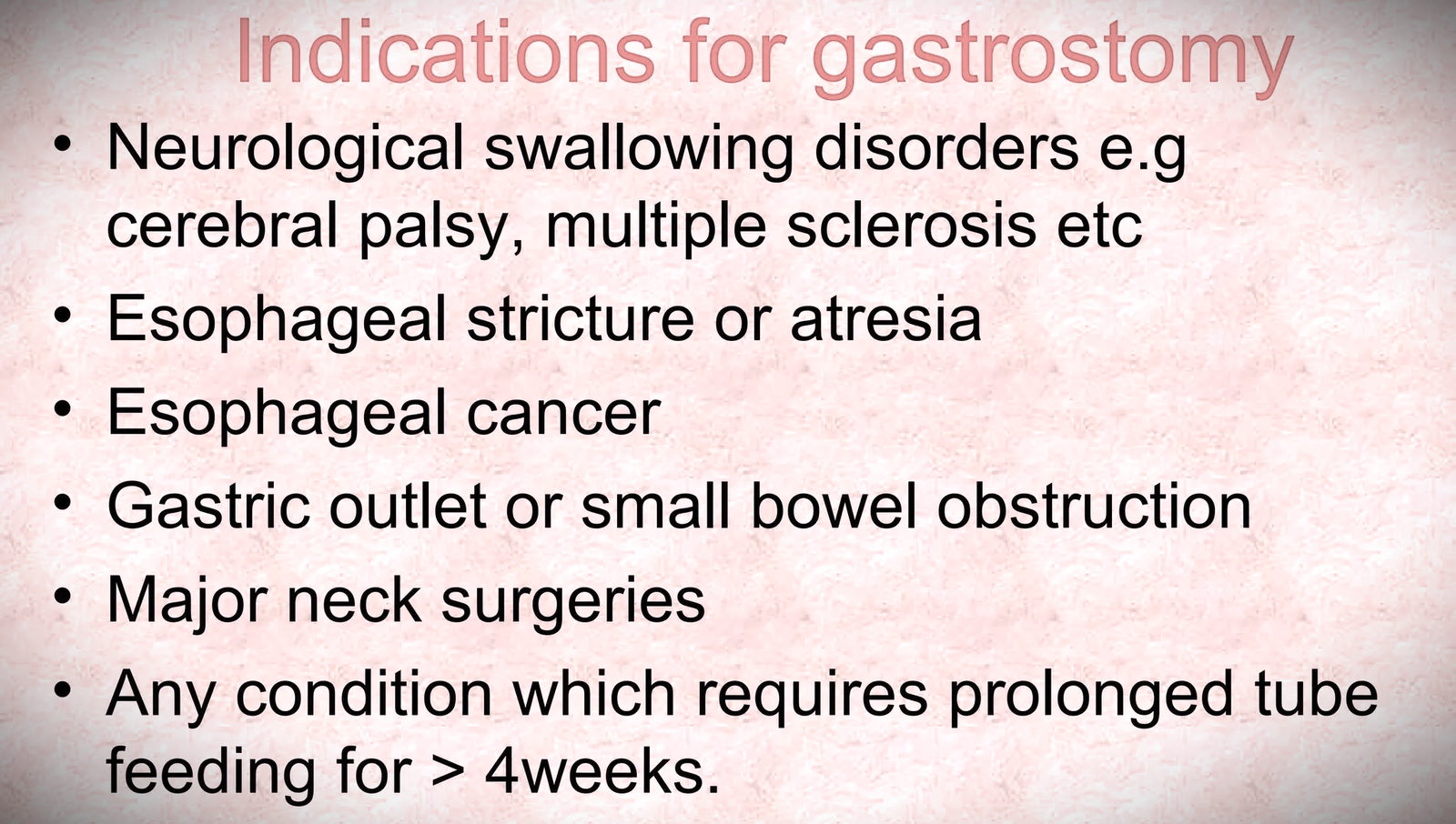
Indications for Gastrostomy Feeding
Gastrostomy feeding may be indicated when a patient has:
1. Impaired Swallowing:
Dysphagia: Difficulty swallowing due to neurological conditions (e.g., stroke, brain injury), muscular diseases, or structural abnormalities of the mouth, throat, or esophagus.
Aspiration Risk: High risk of food or liquids entering the airway, potentially leading to aspiration pneumonia.
Esophageal Obstruction: Blockage of the esophagus due to tumors, strictures (narrowing), or other causes.
Carcinoma of the Esophagus: Cancer affecting the esophagus.
Birth Defects: Congenital abnormalities of the mouth or esophagus that impair swallowing.
Esophageal Atresia: A birth defect where part of the esophagus is missing or closed off.
Problems with Sucking or Swallowing: In patients with debilitating diseases like stroke and dementia
Operations of the Upper Gut: Procedures involving the alimentary canal, mouth, nose, and esophagus.
2. Prolonged Malnutrition or Inadequate Oral Intake:
Chronic Illness: Conditions like cancer, Crohn’s disease, or cystic fibrosis that lead to long-term nutritional deficiencies.
Anorexia Nervosa: An eating disorder characterized by severe food restriction and weight loss.
Severe Weight Loss: Inability to maintain adequate weight and nutritional intake through oral means.
3. Impaired Digestion and Absorption:
Short Bowel Syndrome: A condition where a significant portion of the small intestine is missing or non-functional, impairing nutrient absorption.
Malabsorption Disorders: Conditions like celiac disease that interfere with the absorption of nutrients.
4. Delayed Gastric Emptying:
Gastroparesis: Delayed stomach emptying, often due to nerve or muscle dysfunction.
Medication-Induced: Certain medications can slow down gastric emptying.
5. Altered Level of Consciousness:
Severe Brain Injury: Patients who are unconscious or unable to swallow safely due to a brain injury.
Chronic Vegetative State: A state of persistent unconsciousness with no awareness.
6. Chronic Vomiting or Reflux:
Severe Gastroesophageal Reflux Disease (GERD): Persistent vomiting and acid reflux that lead to malnutrition.
Intractable Vomiting: Persistent vomiting that does not respond to medical treatment.
7. Premature Infants:
Prematurity: Infants born before 37 weeks gestation may have immature digestive systems and require tube feeding.
Failure to Thrive: Infants who are not gaining weight or growing adequately.
Methods of Gastrostomy Feeding
Bolus Feeding: Administration of a specific volume of liquid feed over a short period (e.g., 15-20 minutes), often using a gravity set to control the flow rate.
Continuous Feeding: Delivery of a constant, regulated amount of liquid feed over a longer period using an electronic feeding pump. This method ensures a steady flow of nutrients into the stomach

Types of Feeding Tubes
Feeding tubes are generally categorized by their length and how they are held in place:
A. Long Tubes:
Percutaneous Endoscopic Gastrostomy (PEG) Tube: A long, flexible tube inserted through the abdominal wall directly into the stomach. Placement is achieved using an endoscope – a thin, illuminated tube with a camera – to visualize the stomach and guide the tube into the correct position. This method is less invasive compared to surgical approaches.
Long Balloon-Retained Tube: These are extended tubes featuring a small balloon at the tip. Once positioned in the stomach, the balloon is inflated to secure the tube and prevent displacement. These tubes are often selected for patients who require nutritional support over an extended period.
Malecot Tube: A type of long tube that can be utilized for temporary nutritional support. It is also frequently employed for drainage purposes rather than just feeding.
B. Skin-Level Tubes:
Firm Silicone Mushroom-Retained Tube: These tubes utilize a distal end shaped like a mushroom, designed to rest against the inner stomach wall. This mushroom tip acts as a retention mechanism, minimizing the risk of accidental tube dislodgement. Examples include various brands of button-style feeding tubes.
Balloon-Retained Tube: These tubes incorporate a small inflatable balloon near the tip. After insertion, the balloon is inflated within the stomach to anchor the tube securely. Examples include low-profile gastrostomy tubes that use balloon retention mechanisms.
Procedure for Administration of Gastrostomy Feeding
Preparation (Equipment Tray):
Feeding Administration Set: Including a funnel or feeding syringe, flexible tubing, and a connector (glass or plastic).
Nutritional Feed: Warm feed to body temperature (approximately 37-38°C or 98.6-100.4°F), with a volume of 240-300ml of a liquid, nutrient-rich formula. Maintain the feed’s warmth by placing its container in a basin of warm water.
Protective Drape: A towel and waterproof sheet to protect the patient and bedding.
Warm Water: A container of warm water for rinsing the tube.
Tube Closure Device: A sterile spigot or clamp to seal the feeding tube when not in use, kept in a sterile container.
Bedside Requirements:
Hand washing facilities and soap/antiseptic hand rub.
Privacy screen to ensure patient dignity.
PROCEDURE
Step | Action | Rationale |
|---|---|---|
| 1 | Observe the general rules of nursing procedure. | Ensures adherence to standard protocols and enhances procedural consistency. |
| 2 | Expose the gastrostomy catheter. | To aid easy working and access to the stoma. |
| 3 | Protect the bed linen with a mackintosh and towel. | Prevents soiling of the bed and maintains a clean environment. |
| 4 | Wash hands and check the temperature of the feed. | To prevent the spread of infection and ensure the feed is at a safe and comfortable temperature. |
| 5 | Aspirate and measure the stomach content before giving the feed. | To ensure feeds are absorbed properly and the stomach is not overfilled. |
| 6 | Pinch the proximal end of the gastrostomy tube and connect the funnel after removing the spigot. | To avoid air entry into the stomach, which can cause discomfort or complications. |
| 7 | Pour 10ml of water into the funnel, let it run through the tube slowly, followed by the prescribed amount of feed. Rinse the tube with 10ml of warm boiled water. | To ensure the tube remains patent throughout the procedure and to clear any residual feed. |
| 8 | Pinch and disconnect the funnel when feeding is over and replace the spigot. | To prevent air entry into the stomach and backflow of feed. |
| 9 | If the wound has not yet healed, clean the skin around the tube with normal saline, apply a protective cream like Zinc Oxide, and cover with a dry dressing. | To promote healing and prevent infection around the gastrostomy site. |
| 10 | Record the type, amount of food given, and time. Monitor input and output. | Ensures accurate documentation and monitoring of the patient’s nutritional intake and fluid balance. |
| 11 | Provide oral hygiene, clean equipment, and leave the patient comfortable. | To prevent infection and ensure the patient’s comfort after the procedure. |
| 12 | Clear the trolley and wash hands. | To prevent cross-infection and maintain a clean work environment. |
Complications of Gastrostomy Feeding
Complications associated with gastrostomy feeding can be categorized as follows:
1. Tube-Related Complications:
Tube Blockage (Obstruction): Blockage of the feeding tube due to thick formula, medications, or inadequate flushing.
Incorrect Initial Placement (Primary Malposition): The tube is not positioned correctly in the stomach during the initial insertion.
Intestinal Perforation: Accidental puncture of the stomach or intestinal wall by the tube.
Tube Displacement (Secondary Malposition): The tube shifts out of its intended position within the stomach.
Tube Knotting: The tube becomes tangled or knotted.
Accidental Tube Removal: The tube is unintentionally pulled out.
Tube Damage and Leakage: The tube cracks, breaks, or leaks.
Insertion Site Leakage: Leakage of fluid or stomach contents around the tube insertion site.
Bleeding: Bleeding from the insertion site.
2. Site-Related Complications:
Skin and Mucosal Damage: Erosion, ulceration, or necrosis (tissue death) of the skin or mucous membrane around the stoma.
3. Gastrointestinal Complications:
Intestinal Blockage (Ileus): A blockage in the intestines unrelated to the tube itself.
Gastrointestinal Bleeding: Bleeding from the stomach or intestines.
4. Systemic Complications:
Inadvertent Intravenous Infusion: Accidental administration of the feeding formula into a vein instead of the stomach.
Insertion Site Infection: Infection at the stoma site, characterized by redness, swelling, pain, and/or pus.
Aspiration Pneumonia: Inhalation of stomach contents into the lungs, leading to infection and inflammation.
Nasopharyngeal and Ear Infections: Infections in the nose, throat, or ears, potentially related to the presence of the tube.
Peritonitis: Inflammation of the peritoneum (the lining of the abdominal cavity), often caused by leakage of stomach contents.
Infectious Diarrhea: Diarrhea caused by a bacterial or viral infection.
5. Metabolic Complications:
Electrolyte Imbalances: Disturbances in the levels of electrolytes (e.g., sodium, potassium, chloride) in the blood.
Blood Sugar Fluctuations: High blood sugar (hyperglycemia) or low blood sugar (hypoglycemia).
Vitamin and Trace Element Deficiencies: Inadequate intake or absorption of essential vitamins and minerals.
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowRelated Topics
Foundations of Nursing (III)
- Apply Nursing process to the management of patients
- Administer prescribed medicine appropriately
- Instilling medication (general)
- Blood transfusion
Specialized Nursing Care Procedures
- Perform Shortening and removal of drains
- Perform Colostomy Care
- Prepare Abdominis Paracentesis (Abdominal Tapping)
- Prepare Lumbar Puncture
- Perform Gastrostomy Feeding
- Carry out gastric Lavage
- Perform Tracheostomy Care
- Ophthalmological Care
- Care of the patient`s ears
- Pre-Operative Eye Care
- Ear Care
- Peri-Operative Care:
- Orthopedic Nursing Care
- Prepare for Neurological Assessment
We are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved