Communicable Diseases
ANTHRAX
Table of Contents
Main differences between the three
| Feature | Type A | Type B | Type non A non B( C) |
|---|---|---|---|
| Viruses | RNA picorna virus | DNA Hepadna viruses | Probably 2 types |
| M O spread | Oro-fecal | -Parenteral -Sexual -Vertical transm’n | Oro-feacal Parenteral |
| Incubation period | 15-45days | 29-80days | Not actually known |
| Age of spread | Mostly in children | Mainly adults | All ages |
| Onset | Abrupt | Insidious | Gradual |
| Severity | Mild | Usually severe | Often mild but may be severe |
| Complications | Uncommon | Relatively frequent | Incidence unknown |
| Mortality | Less than 5% | Up to 10% | Unknown |
| Carriers | None | 10% | Frequency/unknown |
Learning Objectives
- Describe the cause, transmission, and epidemiology of anthrax.
- Identify the different clinical presentations of anthrax based on the point of entry into the body.
- Outline the diagnostic investigations and primary aims of anthrax treatment.
- Explain the treatment protocols for anthrax, including drug choices and nursing care.
- Summarize the key prevention and control measures for anthrax in both animals and humans.
- Compare the different types of animal and human vaccines available for anthrax.
Anthrax
- Is a zoonotic disease caused by the bactreria Bacillus anthracis which is a sporeforming G+ve bacilli.
- It is transmitted by the spores of the bacilli which are shed in large nos in the terminal stages of infection hence spread only by a dying or dead host.
- Causative agent may survive for long time in the environment.
Epidermiology
- It is a disease of cattle, goats and sheep.
- It occurs in epidemics.
- It may spread from one area to another especially when animals are moved from one area to another.
- It may present in different ways depending on the part of entry in the body e.g..
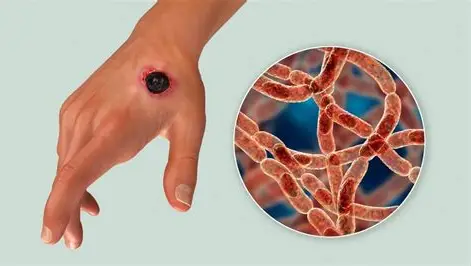
- Anthrax of the skin: common in persons handling cattle, hides and skins, the butchers.
- Anthrax of the lungs: common in people working with infected wool.
- Anthrax of bowel: common in people who eat meat of sick or.
Causes
- Anthrax is caused by a spore forming bacillus called Bacillus Anthracis.
- The spores are formed when the bacillus are exposed to air. Spores are extremely resistant to climatic conditions and can survive for many years in soil.
Clinical picture
o Point of entry – Skin
- Papules
- Blisters
- pustules
- Black central necrosis of pustules
- Extensive edema
- Painless swelling
- Case fatality is mild
o Point of entry -Respiratory tract
- Mild symptoms of URTI- Flu-like symptoms
- Serious respiratory distress- pneumonia
- Shock
- Case fatality is high
on Point of entry – Digestive tract
- Vomiting
- Diarrhea
- Fever
- Sepsis/septicemia
- Abdominal pain
- Case fatality is moderate
Investigations
- Skin– Aspiration of fluid of vesicles for culture.
- Respiratory tract– sputum culture.
- Digestive tract– stool culture.
Treatment Aims
- To prevent spread of infection.
- To treat or prevent shock.
- To treat the cause.
- To prevent complications.
Treatment
- Admit in isolation room and burrier nursing should be emphasized.
- The drugs of choice are the penicillin e.g. Crystalline penicillin.
- Give analgesics to relieve pain.
- Rehydrate the patient especially where there is shock.
- Dressing/cleaning of wounds/ulcer is done daily. All used dressings must be burnt.
- General nursing care.
- DOC Penicillin.
- In severe illness human anthrax immune globulin from vaccinated or recovered individuals.
- Strains resistant to penicillins are used in germ warfare use FLUOROQUINOLONES.
- Prolong antibiotics coz non-germinated spores remain in alveoli for weeks.
Prevention and Control
- Prompt diagnosis and isolation in animals. Cases reported to the public health officers.
- Animals at risk should be vaccinated.
- Carcasses of infected animals should be buried deeply or cremated.
- Humans treated in isolation from other patients.
- Vaccination of those handling animals.
- Vaccination against anthrax is not recommended for travelers.
- The risk of acquiring anthrax from playing with or handling an animal-skin drum is very low. In recent years there have been a few cases of anthrax among animal-skin drum makers. Some of these cases have been fatal.
- Travelers who wish to bring back animal hides from anthrax-endemic regions for the purpose of drum making should strongly consider the health risks before importing animal skins.
- Travelers are warned against having direct or indirect contact with carcasses of animals found in anthrax-endemic regions or consuming meat from animals that were not determined by health officials to be healthy at the time of slaughter.
- Currently, no tests are offered or available to determine if animal products are either contaminated with or free of B. Anthracis spores.
- Animal-skin drum owners or players should report any unexplained fever or new skin lesions to their health-care provider and describe their recent contact with.
Animal vaccine
- The first animal vaccines were developed around 1880 by Pasteur, Toussaint, and Greenfield.
- In 1935 Sterne developed an attenuated live animal vaccine that is still in use and derivatives account for almost all vaccines used in the world today.
- Being a live bacteria, its most significant problem is that it retains some of its virulence. Goats, llamas, and occasionally other animals may die following vaccination.
- However, the benefits far outway the losses, and the vaccine, combined with improved animal husbandry and industrial hygiene, have led to the almost total dissappearence of anthrax in developed countries.
Human vaccines
- There are three vaccines that are commercially available at this time: the georgian/russian, the UK, and the US vaccines.
- All three are derived from an avirulent strain of bacillus anthracis called the sterne strain. This strain lacks the plasmid px02 which encodes the protecive coating of the bacteria.
- The Georgian/Russian vaccine, consists of live spores from the Sterne strain administered in the shoulder by scarification. Its efficacy is unknown but it is reputed to have a high number of side effects and contraindications.
- The UK and US vaccines consist of alum-precipitated cell-free filtrates of bacilli i.e the protective antigen PA.
- Vaccination consists of six initial doses at 0, 2, and 4 weeks and 6, 12, and 18 months followed by a yearly booster. In the UK the first three doses are three weeks apart. As expected, both vaccines manage to increase the bodies response to PA in the form of increased IgG.
- However, despite the name of protective antigen, high antibody levels do not correlate with an immune state. In fact the actual correlate of immunity for anthrax is not known at this time. Antibodies are important but haven’t been the deciding factor in animal models.
- The immunization schedule demonstrates that the vaccine is poor in generating immunological memory.
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowWe are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved