Communicable Diseases
Trypanosomiasis (Sleeping Sickness)
Table of Contents

Learning Objectives
- Describe the definition, etiology, and life cycle of African Trypanosomiasis in both the vector and human host.
- Identify the different forms of the disease, their geographical distribution, vectors, and animal hosts.
- Explain the pathogenesis and pathology of sleeping sickness, including its effects on various body systems.
- Recognize the clinical presentation of the disease through its different stages: chancre, systemic, and cerebral.
- Outline the management of sleeping sickness, including early and late-stage chemotherapy and nursing care.
- List the key methods for the prevention and control of sleeping sickness in affected communities.
TRYPANOSOMIASIS (SLEEPING SICKNESS)
Definition; Is a disease caused by protozoan haemoflagellate trypanosome. Haemoflagellate means a type of protozoa with one or more flagella projecting from its body surface used for swimming in animals/ human blood. It is a parasite in man that is got from animals. Trypanosomiasis is a disease of animals that is transmitted to man by several routes and tsetse flies vector of genus Glossina fly; bites at day light and both sexes carry the infection.
AETIOLOGY Caused by trypanosome flagellates. They have flagella for the movement in blood. They are of different shapes) long and slender) Others are short and slumpy and others are nucleated and antigen coat. Are actively very motile. Live in blood and animal tissues only. Have two life cycles i.e. in an insect vector and the other in animals/ human beings.
FORMS/ TYPES OF TRANSMISSION
- Trypanosome Brucei gambiense (TBg) which may attack humans and found predominantly in west Africa (WA) and West Nile in Uganda.
- Brucei rodensiense which attacks majority of cattle plus sleep and found in East Africa and Central Uganda.
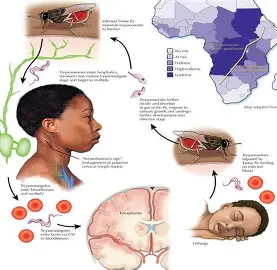
LIFE CYCLE IN THE VECTOR
The long slender infective trypomastigotes forms are taken in by both male and female flies with a blood meal. In the mid gut, the trypanosomes lose their antigenic coat and away take either of these routes. The short circuit route;-The trypomastigotes may penetrate the mid gut wall, from which they can enter the salivary glands direct. Classical route; – The trypanosomes penetrate down the gut to the end of the peritrophic membranes until they reach its posterior end forward up to anterior part of the fly, the salivary glands. In the salivary glands, they change into multiplicative Epimastogotes, then again to trypomastigotes (infective form).
LIFE CYCLE IN MAN
Man is infected by the bite of the tsetse fly with the infective trypomastigotes which are transformed into multiplicative long slender blood forms. They reach the lymphatic and blood circulation that carry them to other organs such as the cells lining up the ventricles of the brain and hide there away from the drugs. Other non-flagellated forms (amastigotes) develop in tissues like the myocardium, they re-enter the blood and cause prolapses. These forms may change to the trypomastigotes which are readily picked up by the tsetse flies during their blood suckling meal.
VECTORS
River Rine type of tsestse fly that breeds along the rivers and lakes and the main type here is glossina palpabis which transmits mainly trypanosomia brucei gambiense. The wounded type. They stay in the open rightly wooded packed land away from water and the main type is glossina marsilans which carries TBr (trypanosome brucei rodesience).
HOSTS
- TBg; Pigs, Dogs, Antelopes, Cows, Sheep, Goats, Human.
- TBr; Antelopes, and pigs, man (man “carriers” the most common cause of infection.
OCCURANCE AND IMPORTANCE
Interference of the economic development of the counties’ in Africa because of trypanosome effects on human and animal population and the disease is invariably fatal if not treated. Incubation period; The fly becomes infected and infective for 2 to 3 weeks after feeding on the infected blood in the TBr and may take months and years in TBg.
Transmission routes
Unusual routes;
- Bite from an infective tsetse fly
- Transplacentally ;- Rare route- but evidences in Germany
PATHOGENESIS
It has been stated that trypanosomes produce toxins that damage the tissues though skin has not been proved. This is responsible for the inflammatory changes seen at primary chancre, skeletal and heart muscles. Toxins may destroy the ependymal cells lining the brain ventricles. This interferes with the release of serotonin which is a neuro A hormone responsible for the maintenance of sleep rhythm causing sleep disturbance. This is done by the trypanosomes releasing “tryptophol” which inhibits serotonin neurotransmission hypersensitivity reaction to the presence of trypanosomes may cause pruritis and urticaria.
PATHOLOGY
- About 300 trypanosomes are needed to cause serious damage.
- They multiply in tissue spaces at the side of the bite (chancre) with local inflammatory reactions such as swelling and mononuclear infiltration.
- Trypanosomes then spread to the lymphatics, lymph glands and blood stream.
- Lymph glands become swollen and fleshy, later hard and fibrotic.
- Slight spleenomegally with rapid multiplication of endothelial cell congestion at the outer layers of the spleen sinuses with localized necrosis from phagocytes.
- Muscle layer plus other layers of the heartall affected.
- Slight spleenomegally with necrosis of central lobules.
- Glomerulo-nephritis of the kidneys results with fibrosis.
- The reticulo-endothelium proliferation in the vessels of the lungs causes blockages fibrosis and collapse of the lung.
- Localized oedema due to collection of lymphocytes e.g. in the eye lids, perineum, skin of the black.
- Serous effusion in the pericardial, pleural and peritoneal caritis.
- Severe anaemia in TBr due to rapid haemolysis of the red blood cells especially, from the lysins produced by the trypanosomes which coat the red blood cells with immune complexes that are circulating, increasing their size. Destruction of leucocytes plus thrombocytes leads to dessiminated intravascular coagulation.
- Brain may be congested and oedematous, dura stuck to the skull and arachnoid matter which increase intercranial pressure (I.C.P) with flat convulsions of ventricles are distended with fluids, blood vessels may be ruptured, ending in intracerebral bleeding, the C.S.F may be invaded too.
CLINICAL PRESENTATION (ACCORDING TO STAGE)
ONSET: Both TBg and TBr run a similar course but TBr is often acute and virulent, ensuring death with 2 to 3 years if not treated.
Primary/ chancre stage.
- History of bite
- Local swelling/ nodule at the site of the bite which may be abnormally hardened. The swelling may be reddened/ erythematous because of blood supply bringing in WBC to the site of the bite.
- The chancre/ swelling looks like a large boil but with relative pain. This may last for 1 to 2 weeks and may resolve.
BLOOD STAGE/ SYSTEMIC STAGE
- Fever (symptom of blood invasion). Occurs at intervals.
- Lymphadenopathy (due to lymphatic spread through the lymphatic vessels and nodes: spleen and cervical lymph nodes.
- Physical weakness, loss of strength accompanied fever.
- Itchy rashes and skin patches (15 to 30cm in diameter) on the chest, back due to hypersensitivity to the trypanosomes lasting 6 to 8 weeeks.
- Dyspnoea from pericardial effusion and C.C.F in chronic illnesss (TBr).
- Hepatomegally from damage on the liver in chronic illness , with jaundice.
- Pitting oedema on the face, lower limbs, eyelids, abdomen due to cardiac failure or kidney damage.
- Neurologic pains, muscle crumps are common.
- Reduced appetite and loss of weight due to constant sleeping with inability to eat.
- Menstrual irregularities due to hormonal interference (amenorrhoea) and importance in men (same reason) plus gynaecomastia.
- Cause of premature births, abortions, still births.
SLEEPING SICKNESS? CEREBRAL STAGE.
- Persistant headache.
- Progressive mental detoriation, depression, and silence and doses not interested in anything including eating which results in wasting and severe weakness.
- Patient lapses into sleep, which is constant and is forced to do any other activity and irritable.
- Has sleep expression on the face slow staggering gate and puffy face.
- Personality changes.
- Speech is slow and slurred
- Patient lapses into convulsions, status epilepticus or coma.
- Saliva dribbles/ drools unattended/ unrestricted.
- Local symptoms and signs such as paralyzed facial palsy, tremors of the limbs and swaying gait are evidenced.
- Patient dies of heart/ brain complication, with no food intake.
DIFFERENTIAL DIAGNOSIS
- Malaria
- TB
- Meningitis
- HIV/ AIDs
INVESTIGATIONS
- Smear from the chancre for checking the trypomastigotes.
- Wet blood smear and thick blood smear for staining.
- Lymphnode aspiration.
- Sub-arachnoid puncture (L.P, C.S analysis) for the presence of the trypomastigotes.
MANAGEMENT
This is based on the findings on the C.S.F treatment is divided into; Early stage and late stage treatment.
CHEMOTHERAPY/ MEDICAL TREATMENT. As in UCG page 53 to 55. Suramin given I.V because it is irritant and painful if I.M given at interval of 3 to 5 days for 6 to 7 doses.
NURSING MANAGEMENT IS SYMPTOMATIC.
- Admission; Complete bed rest
- Treatment; Suramin pentamidine plus metasorprol to kill trypanosomes; hydrocortisone in case of any reaction to drugs or allergies to the parasites.
- Nursing care of a very weak patient. (Unconscious).
PREVENTION AND CONTROL
- Reduction of human tsetse fly contact
- Active screening, case finding and treatment
- Vector eradication using insecticides, sprayed by use of helicopters.
- Clearing of bushes around homes and paths.
- Provision of latrines for refuse (excreta) disposal instead of the bush where tsetse flies are.
PROGNOSIS
- In untreated cases, prognosis is poor especially with CNS involvement.
NB: DRUGS: EARLY STAGE TREATMENT: a. SURAMIN/ BAYER 205 OR ANTRYPOL.
- Test dose given first for fear of hypersensitivity
- Initial test dose= 100mg.
- 250mg, given, followed by 500mg, then a full dose of 1gm, is given if there is no treatment. Children: 20mg/ kg body weight.
- Full dose should be given to persons of good body weight (50kg) and above and in reasonable state of health. (why this is given in early stage of treatment).
- Signs and symptoms; pruritis, urticaria, rashes, conjunctivitis, photophobia, stomatitis, desquamation of skin, etc.
- Needs to be diluted before use (10mls of 10% solution; 1g)
b. Pentamidine
- Needs to be diluted before use.
- This is given I.M, O.D for 7 to 10 days of 3 to 4mg/ kg or 150 to 300mg adult dose (4% + 10%).
- Patients should be injected while lying down because this drug causes immediate hypotension and adrenaline should be at hand.
- Suramin and pentamidine are only effective in the early stage of the disease before there are signs of CNS involvement.
LATE STAGE TREATMENT
a) MELARSOPROL (MEL.B, ARSOBRAL 3.6%)
- Only drug effective in CNS involvement
- It is in ampoules and already in solution form.
- It is very irritant to the skin and tissues and it must be strictly given I.V route.
- The drug is relatively toxic and may produce encephalactic side effects and the patient condition must be improved first before treatment e.g. correction of nutritional and anaemic states.
- Patients should lie down during injection and to remain in bed for 5 hours later.
- It is given after preliminary treatment of blood trypanosomes with Suramin to avoid a jarisch – Herexmer reaction (hyperpyrexia and malaise) which occurs when large numbers of trypanosomes are killed within a short period of time.
- Usual dose = 3.6mg/ kg, and the max. single dose being 5mls.
- It is started on week one; 0.5mls on day one, D1= 1ml, D3 =1.5mls, then rest of 1 week.
- WK2: D3 = 2mls, D3 = 2.5mls, D3 = 3mls, then 1 week of rest period.
- W3: D1 = 3.5mls, D2 = 2.5mls, D3 = 3mls, then I week of rest period.
- W3: D1 = 3.5mls, D2 = 4mls, D3 = 5mls.
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowWe are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved