Gynaecology
Urogenital Fistulas
Table of Contents
Introduction
• In Uganda, maternal mortality ratio is high at 336/100,000 live births.
• For every woman who dies, there are 16 to 20 who suffer lifetime complications, e.g., obstetric fistula, infertility.
• First evidence of obstructed labor was found in the remains of Queen of Egypt, Henhenit in 2050 B.C.
Introduction (Global Context)
• Globally, more than 2,000,000 women live with untreated fistula.
• About 50,000 to 100,000 new cases annually.
• Incidence: 2.1 per 1000 deliveries.
Definitions
Incontinence: The involuntary or inappropriate passing of urine or feces or both, impacting social functioning or hygiene.
Obstetric fistula: Abnormal communication between the vagina and the bladder or rectum.
Pathogenesis of Fistula
• Compression of the fetal head onto the bony pelvis.
• Reduced blood flow to compressed bladder.
• Ischemia.
• Necrosis.
• Formation of fistula occurs 7 to 12 days following delivery.
• Other injuries may include neurologic and gastrointestinal damage.
Fistula Openings
• Ureter to the vagina.
• Bladder to the cervix.
• Bladder to the vagina.
• Urethra to the vagina.
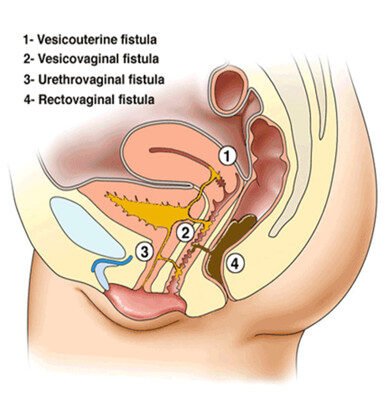
Classification of Obstetric Fistulae
• Vesicouterine fistula (VUF): Between bladder and uterus.
• Vesicovaginal fistula (VVF): Between bladder and vagina.
• Urethrovaginal fistula (UVF): Between urethra and vagina.
• Rectovaginal fistula (RVF): Between rectum and vagina.
• Ureterovaginal fistula: Between ureters and vagina.
Etiologies
• Obstructed labor (>80%).
• Lack of access to emergency obstetric care.
• Iatrogenic causes:
• Caesarean section.
• Assisted vaginal deliveries.
• Total and subtotal abdominal hysterectomies.
• Other causes:
• Radiation.
• Granulomatous diseases (e.g., tuberculosis).
Risk Factors for Obstetric Fistula
• Lack of access to medical facilities, obstetric care, and emergency caesarean section.
• Lack of adequately trained, skilled medical staff.
• Lack of medical supplies and equipment.
• Poverty.
• Malnutrition.
• Early marriages.
• Lack of formal education.
• Cultural beliefs and traditions (e.g., Female Genital Mutilation – FGM).
Diagnosis
• History: Constant leakage of urine from the vagina, History of obstructed labor, Instrumental delivery.
• Physical Examination: Ammonia smell, Excoriation of vulva skin, Recurrent cystitis.
• Investigations: Full Blood Count (FBC), Urinalysis, Serum urea, creatinine, electrolytes.
• Sim’s position: 3 swab test with methylene blue.
Complications of Fistula
• Recurrent fistula.
• Recurrent vaginal and urinary infections.
• Vaginal stenosis.
• Hygiene problems.
• Bladder symptoms.
• Sexual problems.
• Reduced bladder capacity.
Management
Conservative
• Applicable for simple fistula <1 cm.
• Diagnosed within 7 days of occurrence.
• Foley’s urethral catheter.
Surgical
• Repair after 3 months of occurrence.
• Preoperative preparation:
• Nutrition.
• Infection control.
• Dermatitis management.
• Urine acidification.
• Psychological preparation.
Principles of Surgery:
• Wide tissue mobilization.
• Adequate exposure.
• Haemostasis.
• Aseptic technique.
Postoperative Care
• Keep catheter in situ for 14 days.
• Principle of 3 Ds:
• Take fluids.
• Bed dry.
• Catheter draining.
Advice at Discharge
• Delay sexual intercourse for 3 months.
• Pass urine frequently.
• Defer pregnancy for one year.
• Deliver in a hospital.
Prevention of Fistula
Primary Prevention
• Girl child education.
• Women empowerment.
• Collaboration with religious and cultural leaders.
Secondary Prevention
• Avoid obstructed and prolonged labor using a partograph.
• Caesarean section in indicated cases.
• Avoid difficult forceps and destructive deliveries.
• Keep catheter in situ for 7 to 14 days in obstructed labor and bladder repair.
Tertiary Prevention
• Early detection and repair.
• Rehabilitation and integration into the community.
• Family support.
• Delivery in the hospital.
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowWe are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved