Gynaecology
Ovarian Cancer
Table of Contents
Introduction
Ovarian cancer is the second most common gynecological malignancy and the major cause of death from gynecological cancers.
When detected in its early stages, ovarian cancer has an excellent prognosis.
However, the poor overall survival rates reflect the advanced stage at which most women present.
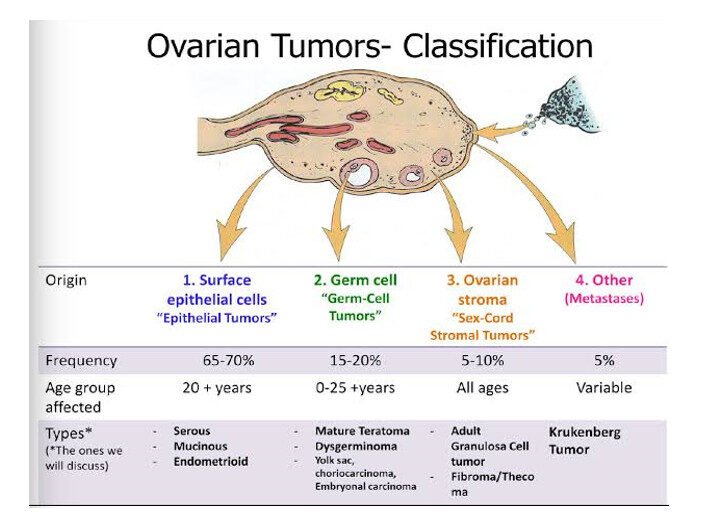
Classification
Epithelial ovarian tumors (80%)
Sex cord stromal tumors (10%)
Germ cell tumors (10%)
Metastatic tumors (including Krukenberg tumors)
Epithelial Ovarian Tumors
Epithelial tumors of the ovary may be benign, malignant, or borderline.
Approximately 10% of epithelial tumors are classified as borderline ovarian tumors (BOTs).
Borderline ovarian tumors (BOTs) are:
Well differentiated, with some malignant features (nuclear pleomorphism and cellular atypia),
But they do not invade the basement membrane.
These tumors may spread to other abdominopelvic structures such as the peritoneum and omentum,
but they rarely recur after initial surgery.
It is estimated that 10–15% of women with epithelial ovarian cancer have a hereditary predisposition.
Women with BRCA1, BRCA2 mutations or Lynch syndrome have an increased lifetime risk of developing epithelial ovarian cancer.
Sex Cord Stromal Tumors
These tumors account for approximately 10% of ovarian tumors,
but represent nearly 90% of all functional (hormone-producing) tumors.
They are generally low malignant potential tumors with a good long-term prognosis.
Some morbidity may occur due to estrogen or androgen production, which can result in:
Precocious puberty
Abnormal menstrual bleeding
Increased risk of endometrial cancer
The peak incidence occurs around the menopausal age,
although juvenile granulosa cell tumors may occur in girls under 10 years, causing precocious puberty.
A significant number of these tumors present with hormonal manifestations, including:
Irregular menstrual bleeding
Postmenopausal bleeding
Precocious puberty in young girls
Germ Cell Tumors
Malignant germ cell tumors occur mainly in young women and constitute about 10% of ovarian tumors.
They are derived from primordial germ cells of the ovary and may contain any cell type.
The management of germ cell tumors primarily focuses on fertility-preserving surgery and chemotherapy.
The most common presenting symptom is a pelvic mass.
About 10% of cases present acutely with torsion or hemorrhage,
and some occur during pregnancy due to their age distribution.
Approximately 70% of germ cell tumors are Stage I at presentation.
Spread occurs via lymphatic or blood-borne routes.
Subtypes of Germ Cell Tumors
Dysgerminomas account for 50% of all germ cell tumors.
Bilateral in 20% of cases.
May secrete human chorionic gonadotrophin (hCG) occasionally.
Endodermal sinus (yolk sac) tumors are the second most common,
accounting for 15% of germ cell tumors.Rarely bilateral.
Secrete α-fetoprotein (AFP).
Present as large solid masses often causing acute symptoms such as torsion or rupture.
Spread (usually to lungs) is a late event.
Immature teratomas constitute 15–20% of malignant germ cell tumors and about 1% of all teratomas.
About one-third secrete AFP.
Occasionally, malignant transformation occurs in a mature teratoma—most commonly to squamous cell carcinoma.
Risk Factors for Ovarian Cancer
Genetic predisposition (BRCA1, BRCA2, Lynch syndrome)
Nulliparity
Obesity
Cigarette smoking (especially for mucinous tumors)
Intrauterine device (IUD) use
Endometriosis
Diagnosis and Investigations
When ovarian cancer is suspected, a Transvaginal Ultrasound Scan (TVUSS) is the initial imaging test of choice
to assess pelvic pathology.
A pelvic mass is characterized by:
Size and consistency
Presence of solid elements
Bilaterality
Ascites
Extra-ovarian disease (peritoneal thickening, omental deposits)
Tumor Markers
CA125 is a non-specific tumor marker elevated in >80% of epithelial ovarian cancers.
However, it is raised in only ~50% of early-stage cancers.
It can also be elevated in benign conditions such as:
Pregnancy
Endometriosis
Alcoholic liver disease
Risk of Malignancy Index (RMI)
The RMI combines:
Menopausal status
Pelvic ultrasound features
CA125 level
It is used to classify pelvic masses into low, intermediate, or high risk of malignancy.
Further Imaging
If pelvic pathology indicates intermediate or high risk, further imaging includes:
Computed Tomography (CT) scan — to assess extra-pelvic disease and staging
Magnetic Resonance Imaging (MRI) — to define tissue planes and operability
Additional Preoperative Investigations
Chest X-ray
Electrocardiogram (ECG)
Full blood count (FBC)
Urea and electrolytes (U&E)
Liver function tests (LFTs)
If the patient presents with gross ascites or pleural effusion, perform:
Paracentesis or pleural aspiration for symptom relief and/or diagnosis.
A sample of the fluid should be sent for cytological examination.
If the diagnosis remains uncertain or primary chemotherapy is being considered (for advanced disease or unfit patients),
a biopsy is needed before treatment — performed either laparoscopically or under ultrasound/CT guidance.
The omentum is usually the preferred biopsy site.
Management
Surgery
Vertical midline incision is used to access all abdominal regions.
Ascitic fluid or peritoneal washings are collected for cytology.
Standard procedure includes:
Total abdominal hysterectomy (TAH)
Bilateral salpingo-oophorectomy (BSO)
Omentectomy
Further debulking may be required, including:
Bowel resection
Peritoneal stripping
Splenectomy
These aim to achieve complete tumor removal.
Lymph node resection is important, especially in early-stage disease, as studies show occult metastasis may occur.
Conservative Surgery
In young patients with early-stage epithelial ovarian cancer who wish to preserve fertility,
conservative surgery can be performed:
Unilateral salpingo-oophorectomy
Omentectomy
Peritoneal biopsies
Pelvic and para-aortic lymph node dissection
Endometrial sampling to exclude a synchronous endometrial tumor
Chemotherapy
Platinum compounds are the most effective agents in treating ovarian cancer.
They act by cross-linking DNA strands, thereby arresting cell replication.
Main Agents
Carboplatin (preferred due to lower renal toxicity and less nausea)
Cisplatin (equally effective but more toxic)
Uses of Chemotherapy
Primary treatment
Adjuvant therapy after surgery
Recurrent disease
Chemotherapy can:
Prolong clinical remission
Improve overall survival
Provide palliation in advanced stages
The first-line combination is usually:
Platinum compound (Carboplatin or Cisplatin)
Paclitaxel
Paclitaxel
Paclitaxel works by damaging microtubules, disrupting cell division.
A known side effect is total hair loss (alopecia), regardless of dose.
Bevacizumab
Bevacizumab is a monoclonal antibody against Vascular Endothelial Growth Factor (VEGF).
It inhibits angiogenesis, the formation of new blood vessels that feed the tumor.
When combined with carboplatin and paclitaxel,
Bevacizumab has been shown to:
Improve recurrence-free survival
Improve overall survival in advanced ovarian cancer
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowWe are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved