Obstetric Anatomy and Physiology
The Umbilical Cord
Table of Contents
Definition
The umbilical cord, or funis, is the lifeline of the fetus. It extends from the placenta to the fetus and transmits the umbilical blood vessels.
Composition and Formation
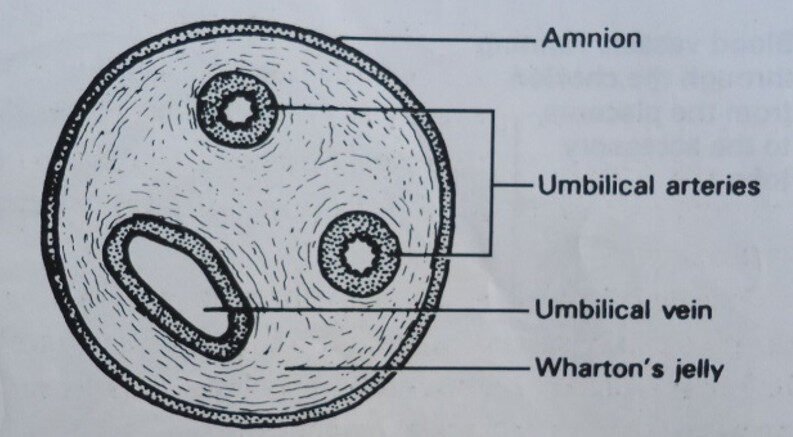
It contains two umbilical arteries and one umbilical vein.
These vessels are enclosed and protected by Wharton’s jelly, a gelatinous substance formed from the mesoderm.
The cord is covered by a layer of amnion, which is continuous with that of the placenta.
It is formed by the 5th week of life.
There are no nerves in the umbilical cord, so cutting it following delivery of the baby is not painful.
Physical Characteristics
Size
Length: The length of the umbilical cord is approximately 50 cm. This is sufficient to allow for the delivery of the fetus without applying any traction to the placenta. A cord is considered to be short when it measures less than 40 cm, but the average is approximately 50 cm.
Diameter: It is approximately 1-2 cm in diameter.
Shape
It has a spiral twist shape.
Abnormalities and Complications of the Cord
Long Cord
Cord Prolapse: The cord can become wrapped around the neck or body of the fetus, which can lead to anoxia (lack of oxygen) in utero.
True Knot: A true knot can form as a result of a long cord. If it tightens, it can cut off blood circulation, leading to Intrauterine Fetal Death (IUD). If it is loose, it may cause asphyxia at birth, leading to a stillbirth.
Short Cord
A short cord can easily break as the baby descends into the pelvis during labor, leading to hemorrhage.
False Knot
These are merely a heaping up of Wharton’s jelly and have no clinical significance.
Very Thick Cord
It is very difficult to clamp and ligature. The midwife has to be very careful.
Very Thin Cord
This can get cut off in the process of the controlled cord traction method of delivering the placenta. This can lead to a retained placenta and subsequently result in Postpartum Hemorrhage (PPH).
Gross Structure of the Cord
Cross-section through the umbilical cord.
Insertion of the Cord
Central Insertion
The cord is commonly inserted in the center of the fetal surface, which is called a central insertion.
Battledore Insertion
The cord is inserted at the edge of the placenta.
Velamentous Insertion
This exists when the cord is inserted 5-10 cm from the edge of the placenta, with the blood vessels running between the placenta and the cord. It is very dangerous if the placenta is situated in the lower segment because the vessels may lie over the cervical os.
Care of the Cord
Immediate Care
Feel for the cord after the delivery of the head.
If it is tight around the baby’s neck, you must clamp it with two clamps and cut it with cord scissors.
If it is loose, you must slip it over the baby’s head.
Proper ligaturing: Apply the first ligature 5 cm from the stump of the baby. Apply a second ligature 2.5 cm from the first one, by use of sterile threads or rubber ligatures.
Check the cord every 10-15 minutes for hemorrhage.
Re-ligature the cord after an hour after the baby is born.
Apply normal saline and keep the cord always dry (spirit is no longer used).
Care in 24 Hours
Keep on observing or checking on the cord; exclude hemorrhage.
Keep the cord clean and dry.
Re-ligature after 24 hours.
Daily Care
The cord is cared for every time. It should be cleaned with normal saline swabs and left dry.
Daily shortening of the cord and re-ligature whenever necessary.
Proper observation to rule out bad healing, such as redness on the cord stump with pus discharge.
A well-treated cord should get off by the 5th day of life.
NB: A thick cord may take longer.
The cord should not be covered by the baby’s clothes.
Avoid applying native medicine.
Dangers of a Neglected Cord
Cord hemorrhage can lead to anemia, and this may result in neonatal death.
If clamped and cut with unsterile clamps or scissors, infections like tetanus can be introduced.
May expose poor healing and separation (i.e., redness, wet cord, and pus).
Low resistance to infection.
Anemia.
Jaundice, which may lead to permanent brain damage in case of kernicterus.
Dehydration.
Omphalitis (infection of the umbilical stump).
Convulsions, which may lead to brain damage.
Septicemia (blood poisoning).
Malnutrition as a result of illness and refusal to breastfeed.
Liver abscess (i.e., microorganisms may enter and cause an abscess).
Death.
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowWe are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved