Obstetric Anatomy and Physiology
SIGNIFICANCE OF THE FEMALE URINARY SYSTEM IN OBSTETRICS
Table of Contents
THE BLADDER
Definition
The urinary bladder is a hollow muscular distensible organ which acts as a reservoir for urine so that it is not passed continuously.
Situation
The bladder lies in the true pelvis with its base resting on the upper ½ of the vagina and the apex pointing towards the symphysis pubis.
Shape
It is like a pyramid when empty but becomes globular as it fills with urine.
Size
About 250-300mls of urine can be contained comfortably in it, but the bladder is capable of greater distension.
Section through the bladder
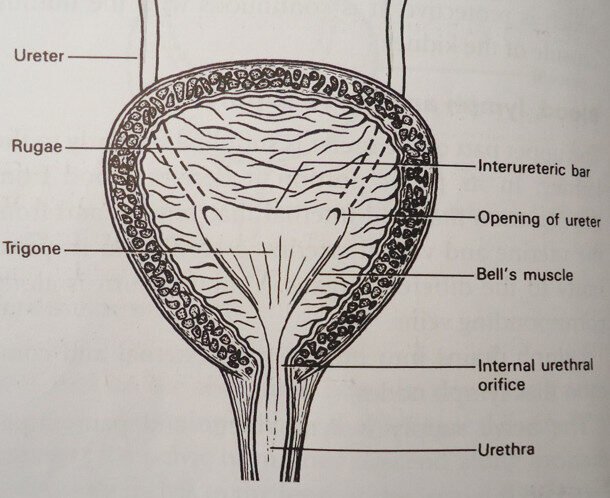
Gross Structure
The bladder consists of the base known as the trigone, an apex pointing towards the symphysis pubis, and a neck which is the point where the urethra enters.
Microscopic Structure
The walls of the bladder are composed of the following layers:
The inner coat: Of transitional epithelium thrown in folds of Rugae to allow distention; this is found lining the cavity of the bladder.
Connecting tissue: It contains the blood vessels, lymphatics, and nerves.
The muscular coat (Destrusor muscles): Consists of three layers of muscles. These muscles are always in a state of painless contraction known as good muscle tone, thus helping the bladder keep the urine inside until it’s ready to be voided. The Destrusor muscles forming the muscular coat of the bladder wall are arranged respectively as follows:
Inner longitudinal layer
Middle circular layer
Outer longitudinal layer
They contract to expel the urine from the bladder. The muscle of the trigone, however, has a special arrangement, passing from the opening of the ureters to the urethral opening.
The outer coat: The upper and outer surface of the rest is covered with peritoneum while the rest is covered with visceral pelvic fascia. Both ureters enter the bladder low on the posterior walls, and the urethra leaves the bladder at its base. They enter obliquely to prevent the backflow of urine.
The Trigone
This forms a triangular structure with equal sides of the triangle being 2.5cm each. It lies inside the bladder cavity and is the most sensitive part of the bladder. Entering obliquely at each upper angle of the trigone are the ureters, which pass about 2cm through the bladder wall.
The urethra leaves from the lower 3rd angle of the triangular epithelium, but it lines smoothly without Rugae because this area does not expand. It is waterproof and very sensitive to infection. The connective tissue lies beneath the epithelium, as it does similarly in the main body of the bladder; it contains lymphatics, nerves, and blood vessels.
The Muscles
The mercer’s bar or intra-ureteric is the muscle lying between the ureteric orifices. It closes the opening of the ureters during micturition to prevent the backflow of urine into the ureters.
The bells muscle extends downwards at each side of the trigone. They extend between the ureteric orifices and the internal meatus of the urethra.
Blood Supply
Inferior and superior vesicle arteries, which are branches from the abdominal aorta.
Lymphatic Drainage
Into external iliac glands.
Nerve Supply
Sympathetic and parasympathetic nerves.
Ligaments
2 Lateral ligaments: from the side walls of the bladder to the side walls of the pelvis.
2 Pubo-vesicle ligaments: from the neck of the bladder to the symphysis pubis.
The urachus: extends from the apex of the bladder to the umbilicus.
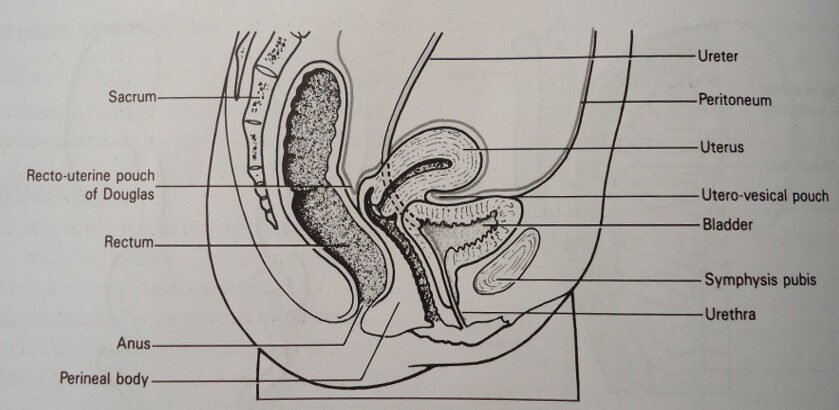
Relations
Anteriorly: Symphysis pubis
Posteriorly: Upper half of the vagina and cervix
Superiorly: Utero-vesicle pouch, body of the uterus.
Inferiorly: The urethra, embedded in the anterior vaginal wall.
Laterally: The pelvic floor muscles.
Sagittal section of the pelvis showing the relations of the bladder
THE SIGNIFICANCE OF THE BLADDER
During Pregnancy
Frequency of Micturition: Is common during the first 12 weeks because during this time the uterus is still a pelvic organ, and so is the bladder. As the uterus grows, there will be no room, and so the bladder is compressed by the growing uterus, causing frequency of micturition.
Physiological changes: Due to hormonal action (progesterone activity) on the muscle of the ureters, making them relaxed and kinked, can also cause frequency.
At 36 weeks: There is frequency again because of the engaging head pressing on the bladder.
Infections: Frequency can also be due to infections like urinary tract infections (UTI), which occur in 2% of all pregnant mothers.
Retention of urine: This can occur around 12 weeks in a retroverted gravid uterus. The growing uterus pulls up the cervix and becomes impacted. The discomfort of this full bladder is only relieved by catheterization.
Incontinence of urine (Stress Incontinence): About the 36th week of pregnancy, as the fetal head engages, urine drips when a patient coughs, sneezes, or laughs.
During Labour
Frequency: In the occipito-posterior position, pressure is exerted on the sacral plexus nerve. This sends stimulus to the nerves of the bladder (sympathetic and parasympathetic) through the Lee-Frankenhauser plexus. Sometimes there is then an urge to pass urine, but the patient is unable to do so.
Retention: Pressure on the sacral plexus can also cause a lack of stimulus to the bladder. During labor, the urethra also stretches from 4cm to 15cm. If the bladder is kept full until labor is well advanced, there are great difficulties in passing urine, and even catheterization is difficult.
Incontinence: If the bladder is not emptied in the first stage of labor, there will be dripping of urine with each expulsive contraction in the 2nd stage of labor.
Complications of a Full Bladder in Labor:
A full bladder causes delay in the 1st and 2nd stage of labour by inhibiting good uterine contractions.
As a result of this delay, there is going to be prolonged pressure of the descending head on the bladder wall. The full bladder will be nipped between the head and the symphysis pubis, causing bruising of the bladder wall.
Then, as the pressure continues, the blood supply will be cut off. As a result, there will be necrosis of that compressed part, leading to slough which can detach and leave a hole known as a vesicovaginal fistula (VVF), causing incontinence of urine.
The urethra is also bruised, potentially causing a urethral-vaginal fistula.
In 3rd stage of labour: A full bladder can cause serious complications, e.g., Postpartum Hemorrhage (P.P.H) and retained placenta. It is therefore very important to keep the bladder empty at all stages of labour.
During the Puerperium
Frequency: Due to polyuria brought about by physiological changes, especially during the first 48 hours. Some of the protoplasm which had grown ten times in thickness and 10 times in width are now broken down and excreted by the kidneys through the bladder in the form of urine. Uterine involution also recurs, leading to frequency of micturition.
Retention: This can occur in cases that are confined to bed. Early ambulation is therefore important. If a patient is not used to a bedpan, she can fail to empty the bladder.
Embarrassment or lack of privacy can also cause retention.
Pain from stitches or a bruised perineum can make a patient fail to pass urine.
Insufficient stimulus due to pressure during labour.
An overstretched bladder during labour may later on lose its muscle tone, leading to retention.
An injury: In the puerperium, the bladder should be palpated so as to detect residual urine which may accumulate and be a predisposing factor to urinary infection due to stasis or stagnation.
Secondary P.P.H: Can be caused by a full bladder.
Incontinence: Due to a major degree of trauma during the 1st and 2nd stage of labour which resulted in V.V.F.
Stress Incontinence
Mechanism of Micturition (Note: Original text labeled this ‘Stress Incontinence’)
The sensation of a full bladder is conveyed to the brain by sensory sympathetic nerves.
Then at a suitable time, the voluntary nerve relaxes the membranous sphincter.
The sympathetic nerve relaxes the internal urethral sphincter.
The parasympathetic nerve causes the Detrusor muscle to contract, and this results in the pulling of the internal urethral meatus by the bell muscles.
Then intra-abdominal pressure is increased, and urine is passed with a bearing-down movement.
THE URETHRA
Definition
This is the channel leading from the bladder to the surface of the body by which the urine is voided.
Situation
It runs from the apex of the trigone to the external anterior vaginal wall.
Shape
It is tubular.
Size
In the female, it is about 4cm (1.5 inches) long but is capable of elongating, as it does during labour when the bladder becomes an abdominal organ. This stretches the urethra to 10cm and makes catheterization difficult. It is introduced in the anterior vaginal walls.
Gross Structure
Internal meatus: Where it meets the neck of the bladder.
External meatus: The opening in the vestibule.
Urethral crypts: Small, blind ducts open from the wall of the urethra. The lowest ones at each side of the urethral orifice are known as Skene’s ducts.
Microscopic Structure
Stratified epithelium lines the lower half of the urethra.
Transitional epithelium lines the upper half.
Connective tissue lies beneath the epithelium.
The muscle coat is arranged in two layers:
Inner layer of longitudinal fibers
Outer layer of longitudinal fibers
The muscle is thickened around the internal meatus to form the sphincter muscle. The external meatus is surrounded by the membranous sphincter.
The urethra needs no outer protection because it is embedded in the anterior wall of the vagina.
Blood Supply
Inferior vesicle arteries and pudendal arteries.
Venous Drainage
By the corresponding veins.
Lymphatic Drainage
By internal iliac glands.
Nerve Supply
Sympathetic nerves to the internal sphincter. The membranous sphincter is under the control of the will and is supplied by the pudendal nerve.
Supports
It is given by the anterior vaginal wall and pelvic floor muscle.
Functions
It forms a canal through which urine can be eliminated from the body.
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowWe are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved