Paediatrics II
Convulsions in the new Born
Table of Contents
Definition
Convulsions, also known as seizures, are involuntary spasmodic contractions of the skeletal muscles due to abnormal electrical activity in the brain.
They represent a malfunction of the brain’s electrical system and are a common neurological presentation in children, particularly during the first two years of life.
The underlying causes are diverse and necessitate a thorough investigation.
Causes
The etiology of convulsions varies significantly depending on the age of the child.
A. Neonates (first 28 days of life)
- Hypoxic-Ischemic Encephalopathy (HIE): Severe lack of oxygen to the brain during birth (e.g., prolonged labour, umbilical cord complications, placental insufficiency) is a leading cause. This can result in brain damage and seizures.
- Intracranial Haemorrhage: Bleeding within the brain (intraventricular haemorrhage, subarachnoid haemorrhage) is common in premature infants and can trigger seizures.
- Infections: Bacterial meningitis (infection of the membranes surrounding the brain and spinal cord) and encephalitis (brain infection) are serious causes of neonatal convulsions. Sepsis (blood infection) can also lead to seizures.
- Metabolic Disturbances: These include:
- Hypoglycemia: Low blood sugar.
- Hypocalcemia: Low blood calcium.
- Hypomagnesemia: Low blood magnesium.
- Hypernatremia: High blood sodium.
- Congenital Malformations: Structural abnormalities of the brain present at birth can predispose to seizures. Examples include malformations of cortical development and vascular malformations.
- Withdrawal Symptoms: Infants born to mothers who used certain drugs (e.g., opioids, alcohol, cocaine) during pregnancy may experience withdrawal symptoms, including seizures.
- Kernicterus: Severe unconjugated hyperbilirubinemia (jaundice) can lead to brain damage and seizures.
B. Older Infants and Children
- Febrile Seizures: These are the most common type of seizure in children aged 6 months to 5 years. They are triggered by a high fever (usually above 38°C or 100.4°F) and are generally benign.
- Infections: Meningitis, encephalitis, and other infections can cause seizures.
- Traumatic Brain Injury (TBI): Head injuries, even minor ones, can lead to seizures.
- Epilepsy: This is a chronic neurological disorder characterized by recurrent seizures. There are many different types of epilepsy syndromes.
- Metabolic Disorders: Similar metabolic imbalances as seen in neonates can also cause seizures in older children. These include inborn errors of metabolism.
- Brain Tumors: Tumors in the brain can cause seizures.
- Stroke: Disruption of blood flow to the brain can result in seizures.
Timing of Onset
The timing of the first seizure can offer clues about the underlying cause.
- First Day of Life: Suggests severe asphyxia or intracranial haemorrhage.
- Second Day of Life: May indicate hypoglycemia or other metabolic disturbances.
- Fifth Day of Life: Could be related to hypocalcemia.
- Second Week of Life: Suggests infection (e.g., meningitis).
Signs and Symptoms of Convulsions
The presentation of a seizure can vary greatly. Signs and symptoms may include:
- Generalized Tonic-Clonic Seizures (Grand Mal): These are the most dramatic type, involving stiffening of the body (tonic phase) followed by rhythmic jerking movements (clonic phase). Loss of consciousness occurs.
- Absence Seizures (Petit Mal): These are brief periods of staring and unresponsiveness, often with subtle motor movements.
- Myoclonic Seizures: Sudden, brief jerking movements of one or more muscle groups.
- Focal Seizures: Seizures that begin in one area of the brain and may or may not spread. Symptoms depend on the location of the seizure focus.
- Infantile Spasms: Sudden, brief contractions of the muscles, often occurring in clusters. This is a serious type of seizure in infants.
Other signs that may accompany a seizure include:
- Cyanosis (bluish discoloration of the skin): Due to impaired breathing.
- Apnea (cessation of breathing): Can lead to hypoxia.
- Loss of Consciousness: Varies in duration depending on the type of seizure.
- Incontinence (loss of bowel or bladder control): Common during tonic-clonic seizures.
- Post-ictal state (period after the seizure): The child may be drowsy, confused, or have difficulty speaking. There may be a headache.
- Fever: Often present with febrile seizures.
- Increased Tone (Rigidity): Stiffening of limbs.
- Abnormal Posturing: Unusual positioning of the body.
- Eye Rolling: Upward deviation of the eyes.
Emergency Care
During a seizure:
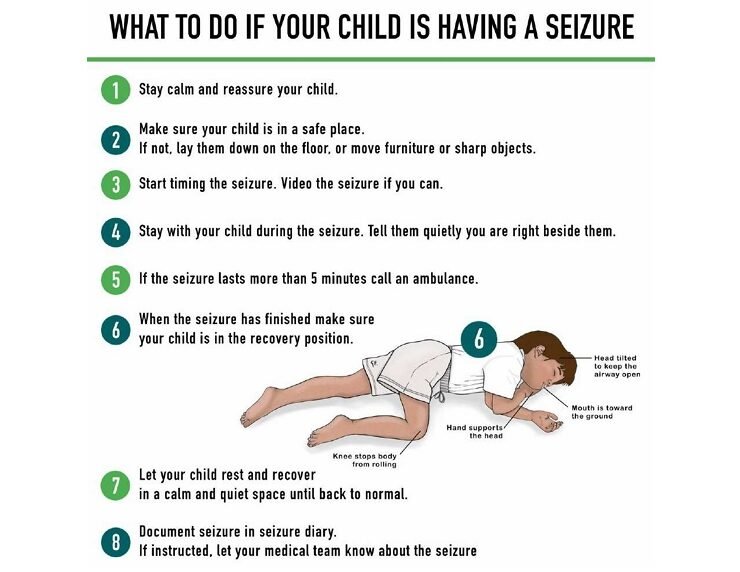
- Safety First: Protect the child from injury by gently placing them on their side to prevent choking on saliva or vomit. Clear the area of any hazardous objects. Do not restrain the child.
- Airway Management: Ensure a clear airway. Turn the child’s head to the side if vomiting occurs.
- Time the Seizure: Note the start and duration of the seizure. A seizure lasting longer than 5 minutes is a medical emergency.
- Monitor Vital Signs: Observe the child’s breathing, heart rate, and skin color.
- Seek Immediate Medical Attention: Call emergency services if the seizure lasts longer than 5 minutes, if the child has difficulty breathing, or if this is the child’s first seizure.
- Do Not Force Open the Mouth: Do not attempt to put anything in the child’s mouth (e.g., spoon, fingers). This is a common misconception and can cause injury.
Hospital Management
Hospital management depends on the cause and severity of the seizures. It may include:
I. Diagnosis
A. History
A detailed history is crucial for determining the underlying cause of the convulsions. Key aspects include:
- Prenatal History: Maternal health during pregnancy, exposure to teratogens (e.g., infections, drugs), and family history of neurological disorders or metabolic diseases.
- Perinatal History: Mode of delivery (vaginal or cesarean), Apgar scores (assessing newborn health at 1 and 5 minutes after birth), birth weight, gestational age, and any perinatal complications (e.g., hypoxia, asphyxia, trauma).
- Postnatal History: Feeding history (breastfeeding or formula feeding), any signs of infections, and developmental milestones.
- Family History: Family history of seizures, epilepsy, or inherited metabolic disorders is important. Also note any family history of sudden infant death syndrome (SIDS).
- Medication History: Maternal drug use during pregnancy (including prescription drugs, illicit substances, and alcohol) and current medications the infant is taking (if any).
B. Investigations
- Laboratory Studies:
- Complete Blood Count (CBC): To evaluate for infection or anemia.
- Blood Culture: To detect bacteremia (bacteria in the blood).
- Urine Culture: To identify urinary tract infection, a potential source of sepsis.
- Cerebrospinal Fluid (CSF) Culture: Essential if meningitis or encephalitis is suspected.
- Serum IgM and IgG Antibody Titers (TORCH): To screen for congenital infections (Toxoplasmosis, Other [syphilis, varicella-zoster, parvovirus B19], Rubella, Cytomegalovirus, Herpes simplex virus).
- Blood Chemistry Panel: Measurement of blood glucose, ammonia, calcium, magnesium, bilirubin, and electrolytes to identify metabolic abnormalities.
- Blood Gas Analysis: To assess for acidosis (excess acid in the blood) and hypoxia (low oxygen levels).
- Imaging Studies:
- Cranial Ultrasound: Especially useful in newborns and infants, to detect intracranial hemorrhage (intraventricular hemorrhage, subarachnoid hemorrhage), cerebral edema, and congenital brain malformations.
- Computed Tomography (CT) Scan: Provides detailed images of the brain to detect structural abnormalities, such as hemorrhage, tumors, or malformations.
- Magnetic Resonance Imaging (MRI): Offers superior soft tissue contrast compared to CT, allowing better visualization of brain structures and detection of subtle abnormalities (e.g., lissencephaly, hypoxic-ischemic encephalopathy, congenital malformations).
- Electroencephalography (EEG): Records the electrical activity of the brain, aiding in identifying the type of seizure, localizing the seizure focus, and assessing prognosis.
II. Treatment
The overall goals of treatment are to:
- Control the convulsions: Stop the seizure activity.
- Stabilize vital functions: Maintain adequate oxygenation, ventilation, circulation, and fluid balance.
- Treat the underlying cause: Address the underlying medical condition causing the seizures.
- Provide supportive care: Ensure adequate nutrition, hydration, and monitoring of vital signs.
A. Controlling Convulsions
- Phenobarbital: Intravenous administration of phenobarbital (20 mg/kg body weight) over 20 minutes is often the first-line treatment for acute seizure control. A maintenance dose (3-4 mg/kg/day) is typically given orally or intravenously for 2 weeks or longer.
- Phenytoin (Dilantin) or Fosphenytoin: If phenobarbital is ineffective, intravenous phenytoin (15-20 mg/kg at a rate of 1 mg/kg/min) or its less irritating formulation, fosphenytoin, may be used. A maintenance dose (3-4 mg/kg/day) is divided and given every 12 hours.
B. Treating Underlying Pathology
The specific treatment will depend on the identified cause:
- Hypoglycemia: Intravenous administration of 10% dextrose (2 mL/kg) over 2-3 minutes, followed by continuous infusion to maintain blood glucose levels between 70-100 mg/dL.
- Hypomagnesemia: Intravenous magnesium sulfate (0.4-0.8 mEq/kg) every 12 hours until magnesium levels normalize.
- Hypocalcemia: Intravenous calcium gluconate (2 mL/kg of 10% solution) over 5 minutes, followed by oral calcium supplementation.
- Infection: Appropriate antibiotic or antiviral therapy guided by culture and sensitivity results.
- Pyridoxine Deficiency: Intravenous pyridoxine (100 mg).
- Increased Intracranial Pressure: Intravenous mannitol (0.5-1 mL/kg of 20% solution) over 30-60 minutes to reduce intracranial pressure.
C. Supportive Care
- Respiratory Support: Oxygen supplementation, mechanical ventilation (if necessary).
- Fluid and Electrolyte Management: Intravenous fluids to correct dehydration and electrolyte imbalances.
- Nutritional Support: Parenteral nutrition (if necessary) to ensure adequate caloric intake.
- Cardiac Monitoring: Continuous monitoring of heart rate and rhythm.
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowWe are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved