Conditions Affecting the Endocrine System
Subtopic:
Acromegaly/gigantism
Table of Contents
Learning Objectives
Explain the pathophysiology of acromegaly and gigantism, including causes like GH-secreting pituitary tumors.
Identify clinical features of GH hypersecretion, such as facial changes, organ enlargement, and metabolic disturbances.
Describe diagnostic methods, including GH blood tests and CT imaging for pituitary adenomas.
Outline medical and surgical management strategies, including use of dopamine agonists, somatostatin analogs, and tumor removal.
Summarize nursing care before and after pituitary surgery, focusing on education, emotional support, and postoperative precautions.
Recognize long-term complications and home care needs, including activity restrictions, medication administration, and follow-up monitoring.
Acromegaly and gigantism
Acromegaly and gigantism, also known as hyperpituitarism, are most commonly caused by the prolonged overproduction of growth hormone (GH), typically due to a GH-secreting tumor in the pituitary gland. Less often, these conditions result from excess growth hormone-releasing hormone (GHRH) secreted by the hypothalamus. As the pituitary tumor enlarges, it can compress nearby structures, potentially leading to:
Underproduction of other pituitary hormones from both the anterior and posterior lobes.
Damage to the optic nerves, resulting in visual disturbances.
The effects of excessive GH include:
Excessive bone growth.
Enlargement of internal organs.
Formation of excessive connective tissue.
Enlargement of the heart and elevated blood pressure.
Reduced glucose tolerance, increasing the risk of diabetes mellitus.
Growth hormone promotes the growth of skeletal and soft tissues. Therefore, an excess of GH leads to gigantism in children and acromegaly in adults.
Gigantism develops before the growth plates (epiphyses) of long bones fuse, resulting in significant increases in height, often reaching 7-8 feet.
Acromegaly occurs after the growth plates have fused, leading to the enlargement of peripheral body parts (acral regions).
Both conditions are almost exclusively caused by a pituitary tumor.
Clinical Presentation of Growth Hormone Hypersecretion
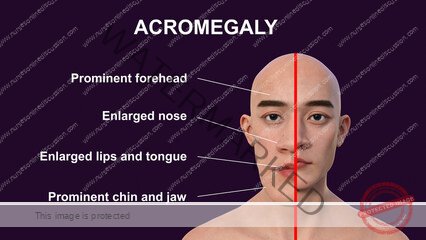
Physical Changes:
Facial changes, including coarsening of features, a broad, thick nose, prominent brow, and spade-like hands.
Elongation and widening of the jawbone (mandible).
Other Signs and Symptoms:
Visual field defects or headaches.
Development of diabetes mellitus.
Hypertension (high blood pressure).
Sleep apnea (interrupted breathing during sleep).
Excessive sweating.
Swelling of soft tissues, such as the lips, tongue, and heel pads.
Tiredness and fatigue.
Weight gain.
Amenorrhea (absence of menstruation) in women.
Shortness of breath.
Pain or tingling in the hands.
Deepening of the voice.
Goiter (enlargement of the thyroid gland).
Muscle weakness.
Joint pain.
Hypopituitarism (deficiency of other pituitary hormones) may also occur.
Diagnosis
Elevated baseline levels of growth hormone in blood tests confirm the diagnosis.
Computed tomography (CT) scan of the brain is performed to identify and assess a pituitary adenoma (tumor).
Medical Management
Medications:
Bromocriptine and Cabergoline: These dopamine agonists can help lower GH levels.
Octreotide: This somatostatin analog is administered via injection to slow down GH production.
Radiation Therapy: Used to suppress the growth of the pituitary tumor.
Surgical Intervention: Surgical removal of the pituitary tumor is often the primary treatment.
Nursing Management of Acromegaly
Preoperative Care:
Provide education about the cause of the disease, the prescribed medical treatment plan, and preparation for surgery.
Offer emotional support and encourage interaction with family and loved ones.
Reassure the patient that treatment can reverse some of the physical changes.
If the patient exhibits signs of distress or maladaptive behaviors, refer them to appropriate mental health resources.
Prepare the patient and family for the surgical procedure, explaining preoperative diagnostic tests and examinations.
For patients undergoing transsphenoidal hypophysectomy (surgery through the nose) or transfrontal craniotomy (surgery through the skull), explain the postoperative need for nasal packing and a “mustache dressing” to collect drainage.
Postoperative Care:
Elevate the patient’s head to promote breathing and drainage.
Discourage coughing, as it can interfere with healing at the surgical site.
Provide frequent oral hygiene and keep the skin dry.
Encourage or assist with range-of-motion exercises to maintain joint mobility.
Encourage ambulation within 1 to 2 days after surgery.
Educate the patient about avoiding activities that increase intracranial pressure during the healing phase, such as vigorous toothbrushing, coughing, sneezing, nose blowing, and bending over.
Discharge and Home Healthcare Guidelines
Referrals:
Refer patients with advanced acromegaly experiencing arthritis and requiring assistive devices for mobility and daily activities to a physical therapist.
Activity Restrictions:
Instruct the patient to avoid activities that increase intracranial pressure for up to 2 months post-surgery.
Toothbrushing can usually be resumed after 2 weeks.
Advise the patient to report any increased nasal drainage.
Explain that incisional numbness and altered sense of smell may persist for up to 4 months after surgery.
Medications:
If octreotide is prescribed, ensure the patient can demonstrate proper subcutaneous or intramuscular injection technique.
Follow-up:
Regular monitoring is crucial for the development of cardiac disease, diabetes mellitus, gallstones, and recurrence of acromegaly symptoms.
Advise the patient to wear a medical identification bracelet indicating their condition.
Complications
Sterility in females and impotence in males.
Impaired learning ability.
Delayed sexual development.
Poor concentration.
Irritability.
Heart disease.
Diabetes mellitus.
Gallstones.
Enlargement of internal organs (e.g., heart, liver).
Increased risk of certain cancers.
Formation of polyps in the colon.
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowRelated Topics
Medical Conditions Affecting the Endocrine System
- Applied Anatomy and Physiology of the Endocrine System
- Acromegaly/Gigantism (Hyperpituitarism)
- Dwarfism (Panhypopituitarism)
- Addison’s Disease (Adrenal Insufficiency)
- Pheochromocytoma
- Cushing’s Syndrome
- Hyperaldosteronism
- Thyrotoxicosis
- Diabetes Mellitus
Conditions Affecting the Nervous System
- Applied Anatomy and Physiology of the Nervous System
- Trigeminal Neuralgia
- Bell’s Palsy
- Parkinson’s Disease
- Spinal Cord Compression
- Transverse Myelitis
Medical Diseases Affecting the Renal System
- Anatomy and Physiology of the Renal System
- Renal Disorders
- Urinary Tract Infections (UTIs)
- Cystitis
- Renal Failure (Acute and Chronic)Nephrotic Syndrome
- Polycystic Kidney Disease (PKD)
- Kidney Stones (Nephrolithiasis)
Conditions of the Lymphatic System
- Anatomy and Physiology of the Lymphatic System
- Lymphedema
- Lymphangitis and Lymphadenitis
- Hodgkin’s Disease
Conditions of the Musculo-Skeletal System
- Anatomy and Physiology of the Musculo-Skeletal System
- Tendonitis
- Rheumatoid Arthritis
- Osteoarthritis
- Gout
- Bursitis
- Ankylosing Spondylitis
- Osteoporosis
- Paget’s Disease
Skin Conditions (Dermatology)
We are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved