Integrated Management of Childhood Illnesses (IMCI)
Subtopic:
Treat the child in IMCI
EXECUTE THE IDENTIFIED TREATMENT STEPS as outlined in the Assessment and Classification chart.
INSTRUCT THE MOTHER ON HOME ADMINISTRATION OF ORAL MEDICATIONS.
For each oral medication prescribed for home use, adhere to the following guidelines. Furthermore, carefully follow the specific instructions provided with each drug’s dosage:
Determine the Correct Medication and Dosage: Ascertain the appropriate drug and dosage based on the child’s age or weight, ensuring accuracy.
Explain the Drug’s Purpose: Clearly communicate to the mother the reason why this specific medication is being prescribed for her child, addressing her potential concerns.
Demonstrate Dosage Measurement: Show the mother exactly how to measure the correct dose of the medication, using the provided measuring tools.
Observe Mother’s Practice: Watch as the mother practically demonstrates measuring a dose herself, correcting any errors and ensuring she is comfortable with the process.
Supervise First Dose Administration: Encourage the mother to give the very first dose of the medication to her child while still at the clinic, allowing for immediate feedback and reassurance.
Provide Clear Administration Instructions: Explain step-by-step how to give the medication at home. Label the medication clearly and package it appropriately for safe transport and storage.
Separate Packaging for Multiple Medications: If multiple oral drugs are prescribed, gather, count, and package each medication separately. This minimizes confusion at home.
Emphasize Completing the Full Course: Stress the critical importance of using all prescribed oral medications – whether tablets or syrup – to finish the entire course of treatment, even if the child starts to appear better. Explain this is crucial to fully resolve the illness and prevent recurrence or resistance.
Verify Mother’s Comprehension: Confirm the mother fully understands all instructions before she leaves the clinic, answering any remaining questions and ensuring confidence in home treatment.
Administer a Suitable Oral Antibiotic as clinically indicated.*
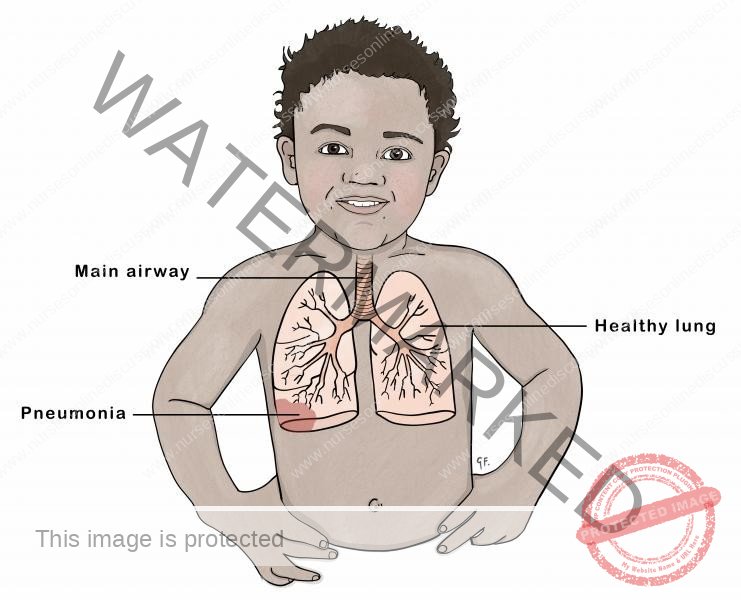
FOR PNEUMONIA, ACUTE EAR INFECTION:
FIRST-LINE ANTIBIOTIC: Oral Amoxicillin
Administer Amoxicillin orally twice daily for 5 days, using the following dosages based on age or weight:
Children aged 2 months up to 12 months (4 – <10 kg):
1 tablet (250 mg)
or 5 ml syrup
Children aged 12 months up to 3 years (10 – <14 kg):
2 tablets (250 mg)
or 10 ml syrup
Children aged 3 years up to 5 years (14-19 kg):
3 tablets (250 mg)
or 15 ml syrup
FOR PROPHYLAXIS IN HIV CONFIRMED OR EXPOSED CHILD:
ANTIBIOTIC FOR PROPHYLAXIS: Oral Cotrimoxazole
Administer Cotrimoxazole orally once a day, starting at 4-6 weeks of age, using the following dosages based on age:
Children less than 6 months: 2.5 ml syrup
Children aged 6 months up to 5 years:
5 ml syrup
or 2 tablets (20/100 mg)

FOR DYSENTERY:
FIRST-LINE ANTIBIOTIC: Oral Ciprofloxacin
Administer Ciprofloxacin orally at a dosage of 15 mg/kg twice daily for a duration of 3 days, using the following age-based recommendations:
Children less than 6 months: 1/2 tablet (250 mg)
Children aged 6 months up to 5 years: 1 tablet (250 mg) or 1/2 tablet (500 mg)
FOR CHOLERA:
FIRST-LINE ANTIBIOTIC FOR CHOLERA: Erythromycin
SECOND-LINE ANTIBIOTIC FOR CHOLERA: Tetracycline
For cholera treatment in children aged 2 to 5 years (weighing 10 – 19 kg), the following antibiotic regimens are recommended:
Erythromycin: Administer 1 tablet (250 mg) four times daily for 3 days.
Tetracycline: Alternatively, administer 1 tablet (250 mg) four times daily for 3 days.
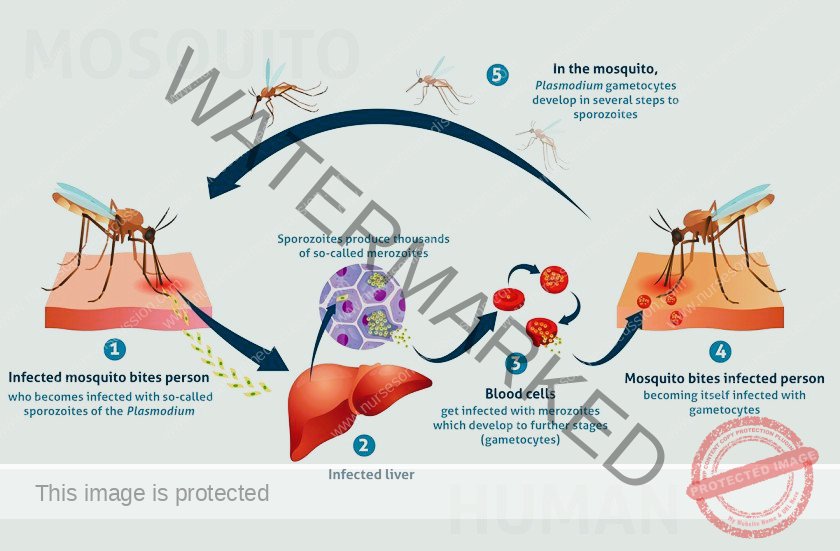
FOR UNCOMPLICATED MALARIA
FIRST-LINE ANTIMALARIAL: ARTEMETHER + LUMEFANTRINE (AL)
SECOND-LINE ANTIMALARIAL: DIHYDROARTEMISININ-PIPERAQUINE (DHA-PPQ)
Artemether + Lumefantrine (AL) Dosage Guidelines:
Dosage is determined by weight or age as follows:
| Weight (kg) | Age (Years) | AL Dosage (Artemether/Lumefantrine) |
| Below 15 | Below 3 | 20mg / 120mg |
| 15 – 24 | 3 – 7 | 40mg / 240mg |
Caregiver Counseling for Malaria Management:
Dispersible Tablet Preparation: Demonstrate the correct way to prepare the dispersible tablet for administration.
Vomiting: Advise that if the child vomits within 30 minutes of dosing, the dose should be repeated. For persistent vomiting, caregivers should seek further medical review.
Dosing Schedule: Clearly explain the dosing schedule and confirm the caregiver’s understanding.
Complete Treatment Course: Emphasize the importance of completing all 6 doses over the full 3-day treatment period, even if the child starts to feel better.
Follow-up: Schedule a follow-up appointment for 3 days after starting treatment.
When to Return Immediately: Instruct caregivers to return to the health facility immediately if the child’s condition worsens or if symptoms continue after 3 days of treatment.
SECOND LINE: DIHYDROARTEMISININ + PIPERAQUINE (DHA-PPQ) Dosage Guidelines:
| Body Weight (kg) | Dose (Dihydroartemisinin + Piperaquine) (mg) |
| 5 to < 8 | 20 + 160 |
| 8 to < 11 | 30 + 240 |
| 11 to < 17 | 40 + 320 |
FOR SEVERE MALARIA
FIRST-LINE TREATMENT FOR SEVERE MALARIA: ARTESUNATE
Artesunate Preparation and Administration:
Artesunate powder is supplied with a 1ml vial of 5% bicarbonate solution for initial reconstitution. This solution is further diluted using either normal saline or 5% dextrose for intravenous (IV) or intramuscular (IM) administration.
| Component | IV | IM |
| Artesunate Powder (mg) | 60mg | 60mg |
| Sodium Bicarbonate (mls, 5%) | 1ml | 1ml |
| Normal Saline or 5% Dextrose (mls) | 5mls | 2mls |
| Artesunate Concentration (mg/ml) | 10mg/ml | 20mg/ml |
Key Notes for Artesunate Use:
Administer Artesunate via IV or IM route for a minimum of the first 24 hours of treatment.
Do not use water for injection for reconstitution or dilution.
Do not use if the prepared solution appears cloudy or contains particles.
Administer Artesunate within 1 hour of preparation to ensure efficacy.
After 24 hours of Artesunate, if the child is able to eat and drink, switch to a full course of Artemisinin-based Combination Therapy (ACT) orally, preferably first-line Artemether Lumefantrine (AL).
Quinine for Severe Malaria:
Intravenous (IV) Quinine Infusion:
Use 5% or 10% dextrose infusion fluids typically.
Administer a minimum of 1ml of IV fluid for every 1mg of quinine.
Do not exceed an infusion rate of 5mg/kg per hour to prevent complications.
Maintain a 1ml fluid to 1mg quinine ratio using 5% dextrose or normal saline for the infusion.
Administer the 20mg/kg loading dose over at least 4 hours.
Administer the 10mg/kg maintenance dose over at least 2 hours.
Intramuscular (IM) Quinine Administration:
Prepare an IM solution by taking 1ml from a 600mg Quinine sulfate IV vial (which contains 2mls) and adding 5mls of water for injection to achieve a 50mg/ml concentration.
For a loading dose, administer 0.4mls/kg IM.
For maintenance doses, administer 0.2mls/kg IM.
If the required dose exceeds 3mls (for loading dose in children >8kg or maintenance dose in children >15kg), divide the dose and administer into two different IM injection sites, ensuring no more than 3mls per site.
Artemether for Severe Malaria:
Administer an initial loading dose of 3.2mg/kg via IM injection immediately, followed by 1.6mg/kg IM daily until the child can tolerate oral medications.
Following IM Artemether, complete the treatment with a full course of oral Artemether Lumefantrine (AL).
Criteria for Admission or Referral for Severe Malaria:
Admit or refer children presenting with:
Severe anemia: Hemoglobin <5g/dl or hematocrit <15%.
Two or more convulsions within a 24-hour period.
Hyperparasitemia with instability. Note: These patients may be treated with AL, DHA-PPQ, or oral quinine if ACT is unavailable, but require close monitoring.
Pre-referral and No-Referral Treatment for Severe Malaria in Children with Very Severe Febrile Disease:
Pre-referral Treatment:
Check availability of pre-referral treatments: rectal artesunate suppositories, injectable artesunate, or quinine.
If rectal artesunate suppositories are available: Insert the first dose immediately and urgently refer the child.
If IM artesunate or quinine is available: Administer the first dose and urgently refer the child to hospital.
If Referral is Not Possible:
For Artesunate Injection:
Administer the first dose intramuscularly.
Repeat the same dose every 12 hours until the child can take oral medication.
Transition to a full course of oral antimalarial as soon as the child can take oral medication.
For Artesunate Suppository:
Administer the first dose of the suppository.
Repeat the same dose every 24 hours until the child can take oral antimalarial medication.
Transition to a full course of oral antimalarial as soon as the child can take oral medication.
For Quinine:
Administer the first dose of intramuscular quinine.
Ensure the child remains lying down for one hour post-injection.
Repeat quinine injection at 4 and 8 hours after the initial dose, then every 12 hours thereafter until the child can take oral antimalarials.
Do not continue quinine injections for more than 1 week.
If malaria risk is low, avoid quinine use in children under 4 months old.
FOR CONVULSIONS
Administer Diazepam to Stop Convulsions
Position the child on their side to maintain an open airway. Ensure the airway is clear. Do not insert anything into the child’s mouth.
Administer 0.5mg/kg diazepam injection solution rectally. Use a needleless syringe (such as a tuberculin syringe) or a catheter for rectal administration.
Check for and address low blood sugar if present.
Provide oxygen support and REFER the child immediately to a higher level of care.
If convulsions persist after 10 minutes, repeat the diazepam dose.
Diazepam Dosage Guide (10mg/2mls Solution)
| Age or Weight | Diazepam Dosage (ml) |
| 2 months – 6 months (5 – 7 kg) | 0.5 ml |
| 6 months – 12 months (7 – <10 kg) | 1.0 ml |
| 12 months – 3 years (10 – <14 kg) | 1.5 ml |
| 3 years – 5 years (14-19 kg) | 2.0 ml |
Note: Dosages are provided in milliliters (ml) and are determined by the child’s weight or age.
For Measles, Persistent Diarrhea, Severe Malnutrition
1. Administer Vitamin A – 3 doses:
For Measles Treatment: Give two doses. Administer the first dose at the clinic and provide a second dose for the mother to give at home the following day.
For Other Conditions: Give a single dose if the child has not received Vitamin A in the past month for these conditions.
For Prevention: Provide a single dose according to the routine Vitamin A supplementation schedule for preventive care.
Administration Method: Cut open the Vitamin A capsule and administer the drops orally.
Follow-up: Instruct the mother to return with the child for the 3rd dose in 2-4 weeks.
Vitamin A Dosage based on Age Range
| Age Range | 200,000 IU Capsule | 100,000 IU Capsule | 50,000 IU Capsule |
| Up to 6 months | Not applicable | 1/2 capsule | 1 capsule |
| 6 months up to 12 months | 1/2 capsule | 1 capsule | 2 capsules |
| 12 months up to 5 years | 1 capsule | 2 capsules | 4 capsules |
For Anemia
Iron and Folate Supplementation Guidelines:
Dosage: Administer iron at a dose of 6 mg/kg daily for a duration of 14 days.
Caution: Avoid iron supplementation in children known to have Sickle Cell Anemia.
Note: Delay folate administration until 2 weeks after completing any sulfa-based drug treatment.
Iron/Folate Tablet Dosage Guide by Age or Weight
| Age or Weight | Ferrous Sulfate 200 mg + 250 mcg Folate | Iron Tablet (200 mg) | Folic Acid Tablet (5 mg) |
| 2 up to 4 months (4 – 6 kg) | – | 1/4 | 1/2 |
| 4 up to 12 months (6 – 10 kg) | – | 1/4 | 1 |
| 12 months up to 3 years (10 – 14 kg) | 1/2 tablet | 1/2 | 1 |
| 3 years up to 5 years (14 – 19 kg) | 1/2 tablet | 1/2 | 1 |
Zinc Sulphate Administration for Diarrhea
Dosage: Administer once daily for 10 days.
Zinc Sulphate Dispersible Tablet (20 mg) Dosage by Age
| Age | Zinc Sulphate Dispersible Tablet (20 mg) |
| 0 months up to 6 months | 1/2* |
| 6 months up to 5 years | 1 |
Dispose of the remaining half tablet of Zinc Sulphate 20mg if using a halved tablet for infants under 6 months.
Deworming
Administer Mebendazole if:
Hookworm and whipworm infections are prevalent in your region.
The child is 1 year of age or older.
The child has not received a deworming dose in the last 6 months.
Mebendazole Dosage:
Children 2 years and older: 500 mg Mebendazole as a single dose in the clinic.
Children under 2 years: 250mg Mebendazole as a single dose in the clinic.
Treating Low Blood Sugar
To Prevent or Treat Low Blood Sugar:
If the child can breastfeed: Encourage the mother to breastfeed immediately.
If breastfeeding is not possible but the child can swallow: Give expressed breast milk or a breast milk substitute. If neither is available, administer sugar water*.
Provide 30 – 50 ml of milk or sugar water* before the child leaves the clinic.
If the child cannot swallow: Administer 50 ml of milk or sugar water* via a nasogastric (NG) tube.
If an NG tube is unavailable: Place 1 teaspoon of sugar moistened with 1-2 drops of water under the tongue (sublingually), and repeat every 20 minutes to prevent recurrence.
Sugar Water Preparation: Dissolve 4 level teaspoons of sugar (20 grams) in a 200-ml cup of clean water.
TEACH THE MOTHER TO TREAT LOCAL INFECTIONS AT HOME
Clearly explain the prescribed treatment to the mother and the reason for its use.
Demonstrate each step of the treatment process. Observe the mother perform the first treatment at the clinic to ensure correct understanding and technique.
Instruct the mother on how frequently to administer the treatment at home.
Confirm the mother’s understanding of all instructions before she departs from the clinic.
Treating Eye Infections with Tetracycline Eye Ointment
Clean both eyes 3 times daily following these steps:
Wash your hands thoroughly.
Ask the child to close their eyes gently.
Use a clean cloth moistened with water to gently wipe away any pus discharge.
Apply tetracycline eye ointment in both eyes 4 times daily following these steps:
Ask the child to look upwards.
Dispense a small amount of tetracycline eye ointment inside the lower eyelid.
Wash your hands again.
Continue treatment until there is no more pus discharge from the eyes.
Advise against using any other eye ointments or drops or inserting any other substances into the eye.
Treating Ear Discharge by Dry Wicking and Ear Drops
Dry Wicking Procedure:
Dry the ear canal at least 3 times daily.
Roll a clean, absorbent cloth or soft, strong tissue paper into a small wick.
Gently insert the wick into the child’s ear canal.
Remove the wick when it becomes wet with discharge.
Replace with a fresh, clean wick and repeat steps until the ear canal is dry.
Ear Drop Administration:
Instill quinolone ear drops (such as ciprofloxacin, norfloxacin, or ofloxacin) after dry wicking three times daily for a duration of two weeks.
Treating Mouth Ulcers with Gentian Violet
Treat mouth ulcers twice daily.
Wash hands thoroughly.
Clean the child’s mouth using a soft cloth wrapped around your finger, moistened with salt water.
Apply half-strength gentian violet (0.25% dilution) to the mouth ulcers using a clean applicator or cotton swab.
Wash hands again.
Continue gentian violet treatment for 48 hours after the ulcers have visibly healed.
Symptomatic Relief
Paracetamol for Pain Relief: Administer paracetamol as needed for pain.
Safe Remedies for Throat Soothing and Cough Relief: Recommend the following safe remedies:
Breast milk for exclusively breastfed infants.
Simple linctus (cough syrup).
Tea with honey (for older children, avoid honey in infants under 1 year old).
Lemon tea.
Treatments to be Given Only in the Clinic
Intramuscular antibiotics (e.g., PPF, CAF) for acute ear infections, very severe disease, and pneumonia.
Quinine for severe malaria cases.
Rectal diazepam for children experiencing convulsions.
Sugar water or milk via nasogastric tube (NGT) for treating or preventing low blood sugar in children unable to swallow.
Treating Thrush with Nystatin
Treat thrush four times daily for 7 days:
Wash hands thoroughly.
Clean the child’s mouth using a soft cloth moistened with salt water.
Administer 1 ml of nystatin solution into the mouth four times a day.
Avoid feeding the child for 20 minutes after medication administration to allow for absorption.
If Breastfeeding: Examine the mother’s breasts for signs of thrush infection. If thrush is present on the breasts, treat with nystatin cream as directed. Advise the mother to wash her breasts after each breastfeeding session.
If Bottle-feeding: Recommend transitioning from bottle-feeding to cup and spoon feeding to reduce the risk of reinfection.
Paracetamol for Pain: Administer paracetamol as needed for pain relief associated with thrush.

TREATMENT OF DEHYDRATION
GIVE EXTRA FLUID FOR DIARRHOEA AND CONTINUE FEEDING
Plan A: Treat Diarrhoea with No Dehydration (Home Treatment)
Counsel the Mother/Caregiver on the 4 Rules of Home Treatment:
Give Extra Fluid: Provide more fluids than usual to compensate for fluid loss.
Give Zinc Supplements (for children aged 2 months up to 5 years): Administer zinc to reduce the severity and duration of diarrhea.
Continue Feeding: Maintain the child’s regular feeding routine to provide nutrition and support recovery.
Know When to Return: Educate the caregiver on danger signs and when to seek immediate medical attention.
1. Give Extra Fluid (Administer ORS and Other Fluids Liberally)
ADVISE THE MOTHER/CAREGIVER:
Breastfeed Frequently and Longer: Encourage more frequent and prolonged breastfeeding sessions.
For Exclusively Breastfed Infants: In addition to breast milk, give Oral Rehydration Solution (ORS).
For Non-Exclusively Breastfed Children: Offer one or more of the following:
ORS solution
Food-based fluids (e.g., soup, enriched porridge (‘bujii’), yogurt drinks, rice water)
Safe, clean water
Provide Potassium-Rich Foods: Offer fresh fruit juice or mashed bananas.
Continue ORS at Home: Instruct caregivers to continue giving ORS as advised, especially:
After Plan B or Plan C treatment at the clinic.
If they cannot return to the clinic if diarrhea worsens.
Teach the Mother/Caregiver How to Mix and Administer ORS:
Provide 2 packets of ORS for home use.
Demonstrate how to prepare and give ORS solution correctly.
Guidance on Extra Fluid Amounts After Each Loose Stool:
| Age Group | Fluid Amount After Each Loose Stool |
| Up to 2 years | 50 to 100 ml |
| 2 years or more | 100 to 200 ml |
Instructions for Fluid Administration:
Give frequent, small sips from a cup.
If vomiting occurs, wait 10 minutes, then resume giving fluids more slowly.
Continue giving extra fluids until diarrhea stops.
2. Give Zinc (for children aged 2 months up to 5 years)
Instruct the Mother/Caregiver on Zinc Administration (20 mg tablet):
| Age Group | Zinc Dosage |
| 2 months up to 6 months | 1/2 tablet daily for 14 days |
| 6 months or more | 1 tablet daily for 14 days |
Demonstrate Zinc Supplement Administration:
Infants: Dissolve the tablet in a small amount of expressed breast milk, ORS, or safe water in a small cup or spoon.
Older Children: Tablets can be chewed or dissolved in a small amount of water.
3. Continue Feeding
If the child is under 6 months old and breastfed, continue exclusive breastfeeding.
4. When to Return
Provide clear instructions on when to return to the health facility for follow-up or if the child’s condition deteriorates.
Plan B: Treat Diarrhoea at Facility with ORS (Some Dehydration)
Administer Recommended Amount of ORS in the Clinic Over 4 Hours:
1. DETERMINE ORS AMOUNT FOR THE FIRST 4 HOURS:
| WEIGHT | AGE (if weight unknown) | Amount of ORS (ml) |
| < 6 kg | Up to 4 months | 200 – 450 |
| 6 – <10 kg | 4 months up to 12 months | 450 – 800 |
| 10 – <12 kg | 12 months up to 2 years | 800 – 960 |
| 12 – 19 kg | 2 years up to 5 years | 960 – 1600 |
Calculation by Weight: An approximate ORS amount (in ml) can also be calculated by multiplying the child’s weight in kg by 75.
Give More if Needed: If the child wants more ORS than the recommended amount, provide additional ORS.
Infants Under 6 Months (Non-Breastfed, with Standard ORS): Give an additional 100 – 200 ml of clean water during this period. This is not necessary if using low osmolarity ORS.
2. SHOW MOTHER/CAREGIVER HOW TO GIVE ORS SOLUTION:
Administer frequent, small sips from a cup.
If vomiting occurs, wait 10 minutes, then continue more slowly.
Continue breastfeeding whenever the child wants.
3. AFTER 4 HOURS:
Reassess the Child: Evaluate the child again and classify the level of dehydration.
Select Appropriate Plan: Determine which treatment plan (A, B, or C) should be continued.
Initiate Feeding: Start feeding the child in the clinic.
4. IF MOTHER/CAREGIVER MUST LEAVE BEFORE 4-HOUR TREATMENT COMPLETION:
Demonstrate ORS Preparation: Show how to prepare ORS solution at home.
Explain Home ORS Administration: Instruct on how much ORS to give at home to complete the 4-hour treatment.
Provide ORS Packets: Give enough ORS packets to finish rehydration, plus 2 additional packets as recommended in Plan A.
Review the 4 Rules of Home Treatment:
Give Extra Fluid
Give Zinc (age 2 months up to 5 years)
Continue Feeding (exclusive breastfeeding if under 6 months)
Know When to Return
Plan C: Treat Severe Dehydration Quickly (Plan C details would follow in the original document, but were not provided in the user’s last input.)
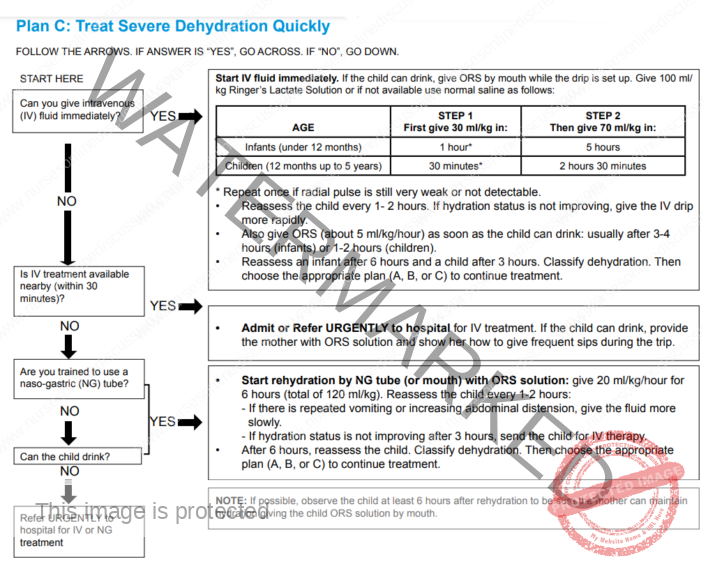
Can You Give IV Fluids?
If YES:
Immediately start IV fluid administration.
If the child is able to drink, give ORS orally while setting up the IV drip.
Administer 100 ml/kg of Ringer’s Lactate Solution. If unavailable, use normal saline. Follow these administration timelines:
Infants (under 12 months):
Step 1: Give 30 ml/kg in 1 hour.*
Step 2: Then give 70 ml/kg in 5 hours.
Children (12 months up to 5 years):
Step 1: Give 30 ml/kg in 30 minutes.*
Step 2: Then give 70 ml/kg in 2 hours 30 minutes.
*Repeat Step 1 once if the radial pulse remains very weak or undetectable.
Reassess the child every 1-2 hours. If hydration is not improving, increase the IV drip rate.
Start oral ORS (approximately 5 ml/kg/hour) as soon as the child can drink. This is usually after 3-4 hours for infants and 1-2 hours for children.
Reassess hydration status after 6 hours for infants and 3 hours for children. Re-classify dehydration and choose the appropriate treatment plan (A, B, or C) to continue care.
If NO (Cannot give IV fluids):
Is IV treatment accessible nearby (within 30 minutes)?
If YES:
URGENTLY Admit or Refer the child to a hospital for IV treatment.
If the child can drink, provide ORS solution to the mother and demonstrate how to give frequent sips during transit.
If NO:
Are you trained to use a naso-gastric (NG) tube?
If YES:
Begin rehydration via NG tube (or orally if possible) with ORS solution.
Administer 20 ml/kg/hour for 6 hours (total 120 ml/kg).
Reassess the child every 1-2 hours.
If repeated vomiting or increasing abdominal distension occurs, reduce the fluid administration rate.
If hydration is not improving after 3 hours, arrange for IV therapy referral.
After 6 hours, reassess the child, classify dehydration, and choose the appropriate plan (A, B, or C) for continued treatment.
If NO:
Can the child drink?
If YES:
Start rehydration orally with ORS solution.
If NO:
URGENTLY Refer the child to a hospital for IV or NGT rehydration.
Treating Shock
Administer a 20 ml/kg bolus of Ringer’s Lactate rapidly (over <15 minutes).
Reassess the child’s condition.
If shock signs persist: Repeat the 20 ml/kg Ringer’s Lactate bolus (<15 minutes) and proceed with Plan C for severe dehydration management (Step 2 onwards).
If shock signs resolve: Treat the child for severe dehydration following Plan C, starting from STEP 2.
GIVE FOLLOW-UP CARE
Provide appropriate care for children returning for scheduled follow-up visits.
For New Problems: If the child presents with any new health issues, perform a complete assessment, classification, and treatment for the new problem.
Condition-Specific Follow-up Checks:
PNEUMONIA: Follow-up after 2 days.
Check for general danger signs.
Assess cough and breathing difficulty.
Ask:
Is the child breathing slower now?
Has the fever reduced?
Is the child eating better?
For any concerns, classify, treat, or refer URGENTLY.
PERSISTENT DIARRHEA: Follow-up after 5 days.
Ask:
Has the diarrhea stopped completely?
How many loose stools per day currently?
For any problems, classify, treat, or refer URGENTLY.
DYSENTERY: Follow-up after 2 days.
Assess for ongoing diarrhea.
Ask:
Are bowel movements less frequent?
Is there less blood in the stool?
Has the fever decreased?
Is there reduced abdominal pain?
Is the child’s appetite improving?
Assess for persistent issues or new problems; classify, treat, or refer URGENTLY as needed.
MALARIA: Follow-up is needed if fever persists after 2 days or recurs after 14 days.
Conduct a full child assessment.
Classify, treat, or refer URGENTLY.
MEASLES: Follow-up after 2 days.
Check for red eyes and pus discharge.
Examine mouth for ulcers.
Check for any unusual mouth odor.
Reassess, classify, treat, or refer URGENTLY.
EAR INFECTION: Follow-up after 5 days.
Reassess the ear problem.
Measure the child’s temperature.
Classify as acute or chronic ear infection; treat or refer URGENTLY.
FEEDING PROBLEM: Follow-up after 5 days.
Reassess feeding practices.
Inquire about feeding issues identified during the initial visit.
Counsel the mother on any new or ongoing feeding problems.
If the child is very underweight for age, schedule a follow-up weight check 30 days after the initial visit.
PALLOR: Follow-up after 14 days.
If not a sickle cell patient, start iron supplementation.
If a sickle cell patient, provide folic acid supplementation.
Advise mother to return in 14 days for further iron or folic acid supply.
Continue iron or folic acid every 14 days for 2 months.
If palmar pallor is still present after 2 months, refer URGENTLY.
VERY LOW WEIGHT: Follow-up after 30 days.
Weigh the child to determine if they are still very underweight for their age.
Reassess feeding practices.
If still underweight, counsel on any feeding problems.
Schedule a follow-up visit in another month.
Continue reassessment and counseling until the child is no longer underweight for age.
If the child is losing weight progressively, refer URGENTLY.
IF ADDITIONAL FOLLOW-UP VISITS ARE REQUIRED based on the initial or current assessment, inform the mother of the next scheduled visit. Also, clearly advise the mother about when to return immediately.
COUNSEL THE MOTHER
FOOD
Assess the child’s current feeding practices.
Inquire about usual feeding habits.
Compare reported feeding to recommended guidelines.
Feeding Assessment Questions:
Breastfeeding:
Do you breastfeed your child?
How many times a day?
Do you breastfeed during the night?
Other Foods/Fluids:
Does the child consume any other foods or fluids?
What types of food and fluids?
How many times per day?
What method do you use for feeding?
(If very underweight) How large are the servings? Does the child have their own serving? Who feeds the child and how?
Feeding Changes During Illness: Has the child’s feeding pattern changed during this illness? If yes, how?
FEEDING RECOMMENDATIONS DURING SICKNESS AND HEALTH FOR CHILDREN UP TO 6 MONTHS OF AGE
Breastfeed frequently, whenever the child desires, day and night, at least 8 times in 24 hours.
Avoid giving any other foods or fluids.
Exceptions: If the child between 4-6 months appears hungry after breastfeeding or is not gaining adequate weight, complementary foods can be introduced (see 6-12 months age recommendations). Introduce these foods 1-2 times per day after breastfeeding.
6-12 MONTHS OF AGE
Continue breastfeeding as often as the child wants.
Provide adequate servings of:
A) Thick porridge: Made from maize, cassava, millet, or soya flour. Enhance with sugar and oil, and mix with milk or pounded groundnuts.
B) Mashed food mixtures: Combine ‘posho’ (maize or millet) or rice or ‘Matooke’, potatoes, or cassava. Mix with fish, beans, or pounded groundnuts. Add green vegetables. Offer snacks like egg, banana, or bread.
Give 3 times daily if breastfed, 5 times daily if not breastfed.
12 MONTHS – 2 YEARS OF AGE
Continue breastfeeding as often as the child wants.
Provide adequate servings of:
Mashed food mixtures based on ‘Matooke’, potatoes, cassava, ‘posho’ (maize or millet), or rice.
Mix with fish, beans, meat, or pounded groundnuts.
Include green vegetables.
Thick porridge from maize, cassava, millet, or soya, with added sugar and oil, and mixed with milk or pounded groundnuts.
Offer snacks like egg, banana, bread, or family food, 5 times a day.
2 YEARS OF AGE AND OLDER
Provide family foods at 3 main meals daily.
Offer nutritious snacks twice daily between meals, such as banana, eggs, or bread.
A good daily diet should be sufficient in quantity and include energy-rich foods (e.g., thick cereal with oil), meat, fish, eggs, fruits, and vegetables.
COUNSEL THE MOTHER ABOUT FEEDING PROBLEMS
If the child’s feeding does not align with the above recommendations, counsel the mother appropriately.
Breastfeeding Difficulties: If the mother reports breastfeeding challenges, assess breastfeeding technique if needed.
Demonstrate correct positioning and attachment for breastfeeding.
Emphasize general breast hygiene before breastfeeding.
Infants Under 6 Months Taking Other Milks or Foods:
Build the mother’s confidence in her breast milk supply adequacy.
Suggest more frequent and longer breastfeeding sessions, day and night, to gradually reduce other milks or foods.
If the mother is working, advise expressing breast milk to leave for the baby.
If other milk is necessary, counsel to continue breastfeeding as much as possible, including at night.
Ensure any other milk is a locally appropriate breast milk substitute, such as cow’s milk.
Verify correct and hygienic preparation and adequate quantities of other milk.
Prepared milk should be consumed within one hour.
Diluted Milk or Thin Porridge:
Remind mothers that infants and young children need energy- and nutrient-dense thick foods.
Advise against diluting milk.
Encourage increasing the thickness of porridge.
Bottle Feeding:
Recommend transitioning from bottle to cup feeding.
Show the mother how to feed the child using a cup.
Passive Feeding:
If the child is not being actively fed, counsel the mother to:
Sit with the child and encourage eating.
Provide an adequate serving on a separate plate or bowl for the child.
Lack of Vitamin A-Rich Foods:
If the diet lacks green leafy vegetables or other vitamin A-rich foods, encourage their frequent inclusion (e.g., green leafy vegetables, carrots, liver).
Delayed Introduction of Complementary Foods (Child 6+ Months):
Gradually introduce thick porridge mixed with a protein source (e.g., milk), plus sugar and fat.
Progressively introduce mashed food mixtures with ‘relish’ (sauce/stew), green leafy vegetables, and fat.
Incorporate nutritious snacks.
Limited Nutrient Density/Variety in Solid Foods (Child eating solids):
Advise on providing a variety of mashed food mixtures using local staples combined with a ‘relish’ made from animal or plant protein.
Ensure inclusion of green leafy vegetables and fat.
Follow-up on Feeding Problems: Schedule a follow-up visit in 5 days for any identified feeding problems.
Fluid Intake During Illness:
Advise increasing fluid intake during illness.
For any sick child, breastfeed more frequently and for longer durations at each feed.
If not exclusively breastfeeding, increase fluid intake with options like rice water, yogurt drinks, or clean water.
For children with diarrhea, extra fluid intake is crucial and potentially life-saving.
Administer fluids according to Plan A, B, or C for dehydration treatment.
Advise the mother about when to return to the health worker for further care.
Follow-up Schedule:
| Condition | Follow-up (Days) |
| Pneumonia, dysentery, malaria, measles | 2 days |
| Persistent diarrhea, acute/chronic ear infection, feeding problem, non-improving condition | 5 days |
| Pallor | 14 days |
| Very low weight for age | 30 days |
Advise on When to Return Immediately:
For any sick child, advise immediate return if:
Not able to drink or breastfeed.
Condition worsens.
Develops a fever.
For a child without pneumonia but with cough or cold, return if:
Fast breathing develops.
Difficult breathing develops.
For a child with diarrhea, return if:
Blood in the stool.
Drinks or breastfeeds poorly.
Counsel the Mother About Her Own Health
If the mother is unwell, provide care or refer her for appropriate treatment.
For breast problems (e.g., engorgement, sore nipples, breast infection), provide care or refer.
Advise on maintaining a healthy diet.
Check her immunization status and administer Tetanus Toxoid (TT) vaccine if needed.
Ensure access to Family Planning (FP) services and Sexually Transmitted Disease (STD)/AIDS counseling/prevention, and antenatal care if pregnant.
We are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved