Eye Conditions
Subtopic:
Eye infection in Children
EYE INFECTIONS
Eye infections arise when pathogenic microorganisms, such as bacteria, viruses, fungi, or parasites, invade the tissues of the eye and its adjacent structures.
Conjunctivitis (Pink Eye): A highly contagious and widespread infection of the conjunctiva, frequently caused by viruses or bacteria. It is common in school settings and easily spreads among children, leading to a characteristic pink or reddish appearance of the eye.
Trachoma: A prevalent infection in certain developing countries and a significant cause of preventable blindness in those regions. It spreads through flies and close contact, and reinfection is a recurring concern. Maintaining hygiene and timely access to treatment are critical for control.
Endophthalmitis: A serious bacterial infection affecting the inner structures of the eye, often occurring after eye surgery or injury, though less frequently. Rapid and potent antibiotic treatment is crucial to prevent potential vision loss. While less common, certain molds can also cause this condition.
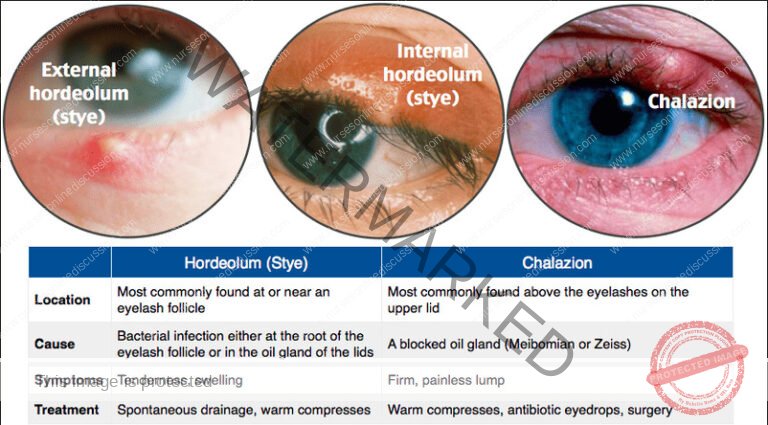
Stye or Chalazion: These are infections or blockages impacting glands within the eyelids. A stye is typically an acute infection of an eyelash follicle or oil gland, while a chalazion is a chronic, painless bump resulting from a blocked oil gland.
Dacryocystitis: An infection of the tear drainage system, specifically the tear ducts, leading to inflammation and obstruction. This can result in excessive tearing and discharge.
Corneal Ulcers: Open sores on the cornea that can be triggered by infections, including bacteria, fungi, viruses, or parasites. Improper contact lens use is a risk factor. Corneal ulcers are serious and require prompt treatment to prevent significant vision impairment.
Orbital Cellulitis: A severe infection affecting the soft tissues surrounding the eye socket (orbit). It is considered a medical emergency demanding immediate treatment to prevent the infection from spreading and causing complications.
Keratitis: Inflammation or infection of the cornea, which can be caused by various pathogens like bacteria, viruses, fungi, or parasites. Symptoms include pain, redness, blurred vision, light sensitivity (photophobia), and corneal clouding.
Blepharitis: Inflammation or infection of the eyelid margins, frequently caused by bacterial infection, seborrheic dermatitis, or blocked oil glands. Common symptoms are crusty eyelids, redness, swelling, burning sensation, and itching.
Uveitis: Inflammation of the uvea, the middle layer of the eye, often linked to autoimmune conditions or infections. Symptoms include eye pain, redness, blurred vision, and sensitivity to light.
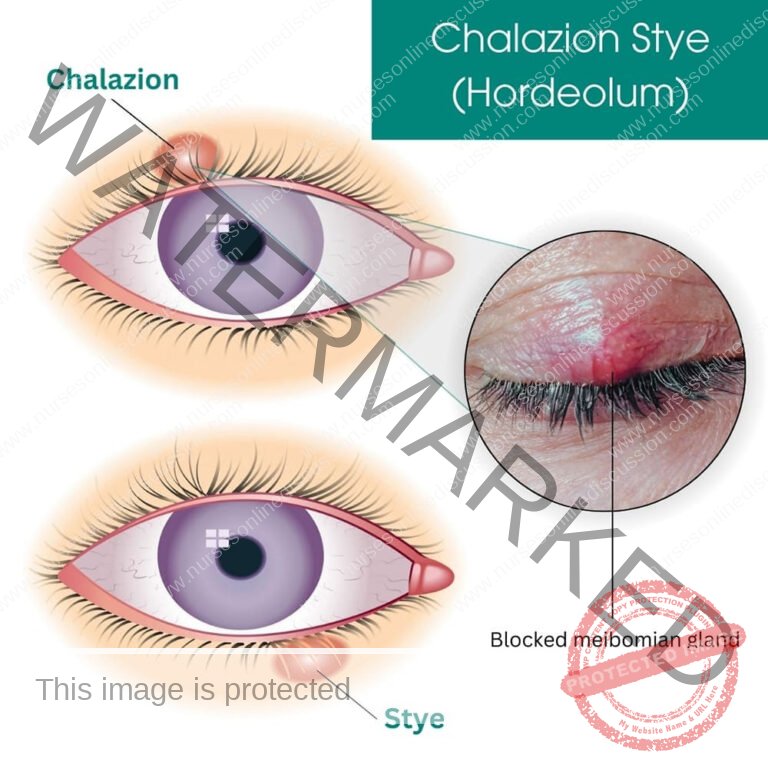
STYE (HORDEOLUM)
A stye, medically termed hordeolum, is a localized infection affecting glands in the eyelid, specifically the hair follicles, sebaceous glands (oil-producing), or sweat glands.
This condition manifests as a painful, bacterial infection or inflammation of the glands or hair follicles situated at the eyelid margin. Staphylococcus aureus is the most frequent bacterial culprit behind stye development.
Styes commonly arise from a Staphylococcus aureus bacterial invasion and can develop in two locations: externally on the eyelid edge, or internally within the eyelid structure itself.
Types of Stye
Internal Hordeolum: This type affects the Meibomian glands located within the eyelid tissue itself.
Clinical Characteristics:
Infection is situated deeper inside the eyelid, often resulting in increased tenderness and pain.
Swelling may extend across a larger portion of the eyelid.
Internal styes can sometimes transition into a chalazion if they become chronic and non-infectious.
External Hordeolum: This involves the glands of Zeis (sebaceous glands) or Moll glands (sweat glands) located at the base of the eyelashes.
Clinical Characteristics:
Appears as a small, red, and painful bump that resembles a pimple along the eyelid edge.
Typically less painful compared to an internal hordeolum.
Often accompanied by localized swelling and redness specifically around the affected area.
Causes of Stye Formation
Bacterial Infection: Staphylococcus aureus is the primary bacterial agent responsible for the majority of stye cases.
Blocked Glands: Obstruction within the eyelid glands (Meibomian, Zeis, or Moll glands) can initiate inflammation and stye development.
Poor Eyelid Hygiene: Inadequate removal of makeup or debris from the eyelid margins can contribute to gland blockage and infection.
Contact Lens Misuse: Improper contact lens practices, such as wearing lenses without proper cleaning or disinfection, can introduce bacteria to the eye area.
Pre-existing Conditions: Certain conditions like blepharitis, rosacea, or seborrheic dermatitis can elevate the risk of developing styes.
Compromised Immunity: A weakened immune system may increase an individual’s susceptibility to bacterial infections, including styes.
Clinical Features
Early Symptoms:
Mild itching or discomfort in the affected eyelid area.
A sensation of fullness or heaviness in the eyelid.
Progressive Signs:
Pain: Localized tenderness and pain, notably intensified upon touching the area.
Redness: Visible inflammation and redness at the eyelid margin or deeper within the eyelid.
Swelling: Puffy, swollen eyelid, which may extend to surrounding areas.
Pus Formation: Development of a yellowish, fluid-filled pustule near the eyelid margin.
Soreness: Persistent irritation and soreness in the affected eyelid region.
Advanced Symptoms:
Drainage of Fluid: Spontaneous rupture of the stye may release yellowish or whitish pus, potentially leading to symptom relief.
Visual Obstruction: Significant swelling can, in some severe cases, partially impede vision.
Management of Stye
General Care:
Avoid Rubbing or Touching the Eye:
Rationale: Prevents introducing additional bacteria and worsening the infection, as well as spreading infection to other eye areas.
Warm Compresses:
Apply a warm compress (clean cloth soaked in warm water) to the affected eyelid for 10-15 minutes, 3-4 times per day.
Rationale: Promotes drainage of pus, alleviates pain, and reduces swelling.
Medications:
Antibiotic Eye Ointments:
Tetracycline 1% eye ointment applied 2-4 times daily, continued for 2 days after symptoms improve.
Rationale: Reduces bacterial load, speeds up healing, and helps prevent further spread of infection.
Analgesics:
Oral pain relievers like ibuprofen or paracetamol for pain management.
Rationale: Helps manage discomfort and swelling.
Eyelash Removal:
Removal of loose or infected eyelashes may be performed by a healthcare professional in certain cases.
Rationale: Prevents recurrent infections by eliminating a potential source of blockage or bacterial growth.
Hygiene Practices:
Clean the eyelid regularly using a sterile saline solution or specialized eyelid-cleaning wipes.
Avoid sharing towels, makeup, or other personal items to minimize bacterial spread.
Lifestyle Modifications:
Maintain proper hand hygiene, especially when wearing and handling contact lenses.
Discontinue makeup use until the stye fully resolves.
Referral to a Specialist:
In cases where the stye does not improve or recurs frequently, referral to an ophthalmologist is recommended.
Persistent or worsening symptoms may require further specialist investigation or intervention.
Potential Complications of Stye
Chalazion Formation: A chronic, painless lump can develop if an internal stye resolves but leaves behind a residual blocked gland.
Preseptal Cellulitis: Infection spreading to the surrounding eyelid tissues, leading to more extensive redness, swelling, and warmth.
Recurrent Styes: Styes that keep returning, especially common in individuals with underlying conditions like blepharitis or rosacea.
Prevention of Stye
Good Eyelid Hygiene: Regularly cleanse eyelid margins using gentle cleansers or diluted baby shampoo and water.
Avoid Eye Contamination: Refrain from touching or rubbing eyes with unclean hands. Avoid using expired or contaminated eye makeup products.
Contact Lens Care: Adhere to proper contact lens hygiene, including thorough cleaning, storage, and timely replacement.
Manage Underlying Conditions: Effectively manage chronic eyelid conditions like blepharitis or seborrheic dermatitis to prevent gland blockages.
Boost Immune Health: Maintain a healthy lifestyle with a balanced diet, adequate hydration, and overall wellness to reduce susceptibility to infections.

TRACHOMA
Trachoma is a persistent infectious condition affecting the external structures of the eye, specifically caused by the bacterium Chlamydia trachomatis. Transmission primarily occurs through close personal contact, such as sharing items like towels and cloths. Additionally, flies that have been in contact with the eyes or nasal secretions of an infected individual can also act as vectors, spreading the bacteria. This infection remains a significant global health concern due to its potential to cause blindness if left untreated.
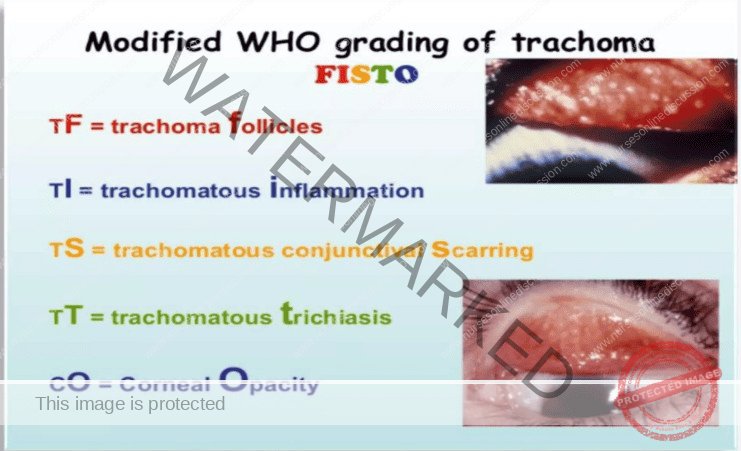
Staging of Trachoma
Trachoma progression is categorized into five stages based on clinical signs in the conjunctiva:
Stage I: Trachomatous Follicles (TF)
Characterized by the presence of five or more follicles in the upper tarsal conjunctiva.
These follicles appear as whitish-grey or yellowish elevations, exhibiting a paler color compared to the surrounding conjunctival tissue.
Stage II: Trachomatous Inflammation – Intense (TI)
In this stage, inflammatory thickening becomes apparent in the upper tarsal conjunctiva.
The conjunctiva appears red, rough, and thickened.
Normal blood vessels, which are usually visible, become obscured due to diffuse inflammatory infiltration and the presence of follicles.
Stage III: Trachomatous Scarring (TS)
Follicles begin to resolve and are replaced by scar tissue.
These scars manifest as white lines, bands, or patches within the tarsal conjunctiva.
Stage IV: Trachomatous Trichiasis (TT)
Arises due to the presence of multiple scars in the conjunctiva.
Scarring causes distortion, leading to inward turning of the eyelid margin (entropion).
Consequently, the eyelashes rub against the cornea, causing corneal abrasions and persistent inflammation.
Stage V: Trachomatous Corneal Opacity (CO)
Represents the advanced stage where the cornea is affected.
Repeated corneal trauma from eyelashes leads to progressive loss of corneal transparency.
This corneal opacity results in visual impairment and potential blindness.
Treatment and Management of Trachoma
Community Diagnosis: Identifying the prevalence of trachoma within a community is crucial for public health initiatives. Understanding the extent of the problem is essential for implementing effective control strategies. The SAFE strategy is a globally recognized approach to combat trachoma in endemic regions.
The SAFE Strategy: This comprehensive strategy encompasses four key components:
Surgery (S) for Trachomatous Trichiasis: Trachomatous trichiasis is the blinding phase of trachoma, where inturned eyelashes cause constant corneal irritation, pain, and light sensitivity. Surgical intervention is vital to correct eyelid malposition and redirect eyelashes away from the cornea, preventing further corneal damage and visual loss.
Antibiotics (A): Antibiotic medications, particularly azithromycin, are a cornerstone of trachoma control. Azithromycin is highly effective in eliminating Chlamydia trachomatis infection. Mass drug administration (MDA) of azithromycin in communities is a key strategy to reduce the infectious reservoir and prevent trachoma transmission.
Facial Cleanliness (F): Promoting facial hygiene is an essential preventive measure to interrupt trachoma transmission. This involves regular face washing, especially focusing on the eyes and nose, using clean water and soap. Consistent facial cleanliness helps remove ocular and nasal discharge, reducing the spread of infection.
Environmental Improvement (E): Enhancing environmental sanitation plays a critical role in reducing trachoma prevalence. Improving access to clean water and sanitation facilities directly impacts hygiene practices and reduces disease transmission. Environmental measures aim to provide communities with clean water sources, proper sanitation infrastructure, and hygiene education.
Treatment by Stage:
Stages I and II:
Antibiotic Therapy: Treatment of choice involves antibiotics.
Azithromycin orally (PO):
Children and adults may receive a single oral dose of azithromycin. Dosage is weight-based for children.
If azithromycin is not suitable, topical tetracycline 1% eye ointment applied twice daily for 6 weeks can be used. For children under 6 months or 6 kg, erythromycin PO may be considered.
Hygiene Education: Emphasize facial cleanliness and hygiene practices.
Stage III:
No specific treatment is typically indicated for trachomatous scarring in the absence of active inflammation or trichiasis. Management focuses on prevention of progression.
Stage IV:
Surgical Treatment: Surgery is the definitive treatment for trachomatous trichiasis to prevent blindness.
Eyelid Surgery: Procedures aim to reposition the eyelashes so they no longer touch the cornea.
Taping: While awaiting surgery, and if regular follow-up is possible, taping eyelashes to the eyelid can be a temporary measure to protect the cornea. This is a palliative approach, not a permanent solution.
Epilation (eyelash removal): Removing ingrowing eyelashes provides only temporary relief, as eyelashes often regrow and can be more abrasive to the cornea upon regrowth. Thus, it’s generally not recommended as a primary treatment.
Stage V:
No treatment can reverse established corneal opacity and blindness. Prevention of progression to this stage is paramount.
Prevention:
Improved Hygiene Practices:
Promote regular face washing, particularly in children, using clean water and soap.
Encourage the use of clean and individual towels and personal washing items to avoid sharing and cross-contamination.
Educate on proper disposal of nasal and eye secretions to minimize environmental contamination.
Access to Clean Water and Sanitation:
Improve community access to safe water sources for drinking, washing, and hygiene practices.
Ensure availability of proper sanitation facilities, including toilets and latrines, to reduce environmental contamination and fly breeding.
Environmental Improvement:
Implement strategies for fly control through environmental management, such as proper waste disposal and fly traps.
Reduce overcrowding in households and communities to minimize close contact and transmission risk.
Improve housing conditions to minimize dust and dirt accumulation, which can harbor bacteria and attract flies.
Antibiotic Treatment Strategies:
Administer antibiotics, such as azithromycin, to affected individuals and communities in endemic areas to treat active infection.
Implement mass drug administration (MDA) programs in trachoma-endemic regions to treat and prevent trachoma on a large scale.
Surgical Intervention:
Provide access to surgical treatment for advanced trachoma, specifically trachomatous trichiasis, to prevent corneal damage and blindness.
Surgery to reposition eyelashes is crucial in preventing vision loss in TT cases.
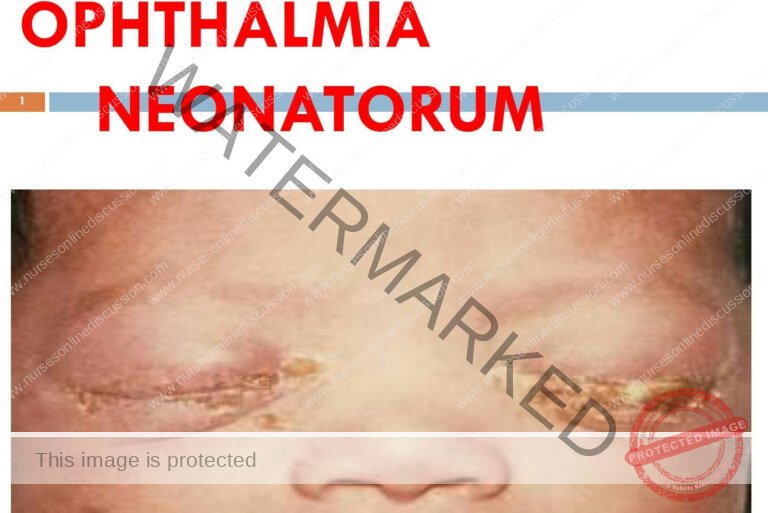
OPHTHALMIA NEONATORUM
Ophthalmia neonatorum, also known as neonatal conjunctivitis, refers to any eye infection occurring within the first 28 days of a newborn’s life.
Flowchart 1: Etiology of ophthalmia neonatorum.
[Flowchart Description: The flowchart visually categorizes the causes of ophthalmia neonatorum into Bacterial, Chemical, and Viral etiologies. Bacterial causes are further divided into Sexually Transmitted (Chlamydia trachomatis, Neisseria gonorrhoeae) and Non-sexually Transmitted bacteria (Staphylococcus aureus, Streptococcus species, Haemophilus influenzae, Pseudomonas, and other species). Chemical causes include 1% silver nitrate solution, topical erythromycin, and gentamicin prophylaxis. Viral causes are listed as Adenovirus, herpes simplex, and enterovirus.]
Pathophysiology:
Inflammation of the conjunctiva leads to redness, dilation of blood vessels, tearing, and discharge. This inflammatory response is often more pronounced in newborns because of factors such as reduced tear production, immature immune system function, lower levels of protective lysozyme activity, and the limited presence of lymphoid tissue within the conjunctiva. Furthermore, newborn tears lack significant levels of immunoglobulin IgA, a key antibody in mucosal immunity.
Etiology:
Bacterial Infections: Bacterial pathogens are a primary cause of septic neonatal conjunctivitis. Historically, Neisseria gonorrhoeae was the most prevalent bacterial agent, typically associated with sexually transmitted infections in the mother. Other bacterial causes include:
Chlamydia trachomatis (most frequent overall): Onset typically between 5-14 days after birth.
Neisseria gonorrhoeae: Usually presents earlier, between 3-5 days after birth.
Staphylococcus aureus
Pseudomonas aeruginosa
Streptococcus species (including S. haemolyticus, S. pneumoniae)
Other bacterial organisms like Klebsiella, Proteus, Enterobacter, Serratia, and Eikenella corrodens.
Viral Infections: Viruses can also induce ophthalmia neonatorum, although they are less common than bacterial causes. Viruses known to cause neonatal conjunctivitis include herpes simplex virus, adenovirus, and enteroviruses.
Chlamydial Infection: Chlamydia trachomatis is a sexually transmitted bacterium that can be passed from mother to infant during childbirth. Infants born to mothers with untreated chlamydial infection have a significant risk (30-50%) of developing ophthalmia neonatorum. Chlamydia trachomatis can also colonize the respiratory system, potentially leading to pneumonia in some infants.
Chemical Conjunctivitis: Aseptic neonatal conjunctivitis can result from exposure to certain chemical agents. Historically, silver nitrate solution was used for prophylaxis against gonococcal ophthalmia, but it has been largely replaced by erythromycin ointment or povidone-iodine in many settings. Chemical conjunctivitis is now less frequently observed due to this shift in prophylactic practices.
Presentation/Clinical Manifestations of Ophthalmia Neonatorum:
Clinical signs and symptoms can vary depending on the specific causative agent, but common features generally include:
Eyelid Swelling: Often the initial presenting sign, with severity ranging from mild eyelid puffiness to significant edema that can make opening the eyes difficult.
Discharge:
Purulent discharge (thick, yellow-green) is typically associated with bacterial infections.
Chlamydial infections may initially present with a less purulent, watery discharge that can subsequently become purulent over time.
Conjunctival Redness (Hyperemia): The conjunctiva appears inflamed and noticeably red.
Photophobia (Light Sensitivity): The infant may exhibit increased crying or discomfort when exposed to bright light.
Corneal Involvement: In severe cases, the cornea (the transparent front surface of the eye) can become cloudy or ulcerated, potentially leading to permanent visual impairment or blindness. This is particularly concerning with gonococcal infections.
Bilateral Symptoms: Typically affects both eyes.
Eyelid Edema: Swelling of the eyelids can hinder proper examination of the ocular surfaces.
Mucopurulent Conjunctivitis: Characterized by discharge that transitions from watery to increasingly purulent, especially in chlamydial infections.
Conjunctival Edema (Chemosis): Swelling of the conjunctiva itself.
Conjunctival Pseudomembrane: In severe cases, a false membrane may form on the conjunctival surface.
Corneal Involvement: Particularly prominent in Neisseria gonorrhoeae infections, potentially leading to corneal perforation.
Epithelial Edema, Superficial Keratitis, and Possible Corneal Ulceration: Signs of corneal surface damage.
Ophthalmia Neonatorum: Prevention and Management
Prevention: Preventive strategies are focused on minimizing the risk of infection before, during, and after birth.
1. Antenatal (During Pregnancy):
Regular Screening for Vaginal Infections: Implement routine screening during prenatal care to detect vaginal discharges indicative of infections such as gonorrhea and chlamydia.
Treatment of Vaginal Infections: Ensure prompt and appropriate antibiotic treatment for any identified vaginal infections in pregnant women using suitable antibiotics.
Management of High-Risk Pregnancies: Address conditions during pregnancy that may elevate the risk of premature labor or prolonged rupture of membranes.
Prevention and Management of Anemia: Manage maternal anemia, as it can compromise the maternal immune system, potentially increasing the risk of infection.
Health Education: Educate expectant mothers on the importance of hygiene practices, including handwashing, perineal hygiene, and avoiding unnecessary touching of the eyes.
2. Intrapartum (During Labor):
Sterile Technique: Maintain strict sterile protocols during labor and delivery. All healthcare personnel should adhere to thorough hand hygiene practices.
Avoid Unnecessary Eye Swabbing: Routine swabbing of the newborn’s eyes during delivery should be avoided unless clinically indicated, as this can introduce infection. If swabbing is necessary for assessment purposes, use separate sterile swabs for each eye, and cleanse from the inner canthus outwards.
Isolation of Infected Mothers: Isolate mothers with purulent vaginal discharge to minimize the risk of transmission to the newborn.
Prophylactic Antibiotics for Prolonged Rupture of Membranes: Consider prophylactic antibiotics for mothers experiencing prolonged rupture of membranes (PROM) exceeding 12 hours to reduce the risk of neonatal infection.
3. Postnatal (After Birth):
Hand Hygiene: Healthcare providers must practice thorough handwashing before and after handling newborns.
Eye Cleaning: Cleanse the baby’s eyes with sterile water or half-strength sterile saline solution using a separate sterile cotton swab for each eye, cleaning from the inner to the outer canthus. Discard swabs after each use.
Avoid Contact with Birth Fluids: Prevent the baby’s face from direct contact with amniotic fluid or other birth fluids.
Educate Mothers: Instruct mothers on proper hand hygiene before handling the baby and to avoid touching the baby’s eyes unnecessarily.
Prophylactic Eye Drops (During Epidemics): In regions experiencing outbreaks of ophthalmia neonatorum, consider using prophylactic eye drops (e.g., 1% silver nitrate or 10% sulfacetamide) immediately after birth. This practice is debated and necessitates careful consideration of potential side effects and local guidelines.
Management of Ophthalmia Neonatorum
Aims of Management:
The primary goals for managing ophthalmia neonatorum are:
Eliminate Infection: To completely eradicate the causative pathogen.
Prevent Corneal Damage: To avoid injury and scarring of the cornea.
Preserve Vision: To protect and maintain the infant’s eyesight.
Prevent Transmission: To stop the spread of infection to others, including family members.
Management in a Maternity Centre (For Mild Cases ONLY – Referral is Usually Necessary):
Admission and Isolation: Admit the infant and implement isolation measures to prevent further spread of infection. Position the baby on their side, ensuring the affected eye is facing downwards to aid drainage. Utilize mosquito nets for protection from flies. Ensure all used materials are kept separate and properly disinfected before laundering.
Eye Cleaning: Regularly cleanse the eyes using normal saline or cooled, sterile boiled water, employing a fresh sterile swab for each eye to prevent cross-contamination.
Topical Antibiotics: Administer antibiotic eye ointment (such as tetracycline or erythromycin) to both eyes, even if only one eye appears to be infected. If ointments are unavailable, consider using diluted crystalline penicillin, following the dosage instructions provided below.
Dosage of Diluted Crystalline Penicillin (When Ointments Are Not Available – ONLY under direct medical supervision, and ideally as a temporary measure prior to hospital transfer):
100,000 IU vial: Dilute with 4 ml of sterile water. Instill 5 drops into each eye every 5 minutes for the initial 30 minutes (6 applications), then 5 drops every 10 minutes for the next hour (6 applications), followed by 5 drops every 30 minutes for 3 hours (6 applications), and finally 5 drops every hour for a total of 3 days.
500,000 IU vial: Dilute with 20 ml of sterile water. Adjust the dosage proportionally to maintain the intended concentration.
Systemic Antibiotics: (Use with extreme caution, and only when hospital referral is significantly delayed and under strict medical supervision). Consider intramuscular crystalline penicillin at a dosage of 50,000 units/kg of body weight every 12 hours for 7 days. This should be considered a last resort and is only acceptable if hospital transfer is delayed, and a qualified medical professional has assessed the situation and is closely monitoring the infant’s response to treatment.
Referral: Refer the infant to a hospital for a definitive diagnosis (including gonorrhea testing, culture and sensitivity tests) and appropriate treatment as soon as possible.
Referral: Refer all suspected cases of ophthalmia neonatorum, especially those exhibiting purulent discharge or corneal involvement, to a hospital without delay.
Assessment and Referral: Conduct a thorough examination of the infant’s eyes. Any infant suspected of having ophthalmia neonatorum, particularly with purulent discharge or corneal involvement, necessitates immediate referral to a hospital equipped with ophthalmology services. Avoid attempting to manage significant cases within a maternity center setting.
Initial Cleaning (before referral): Gently cleanse the eyes with sterile saline or sterile water to remove excessive discharge prior to referral. Utilize a separate sterile cotton swab for each eye.
Management in Hospital:
Diagnostic Testing: The attending physician will order an eye swab for culture and sensitivity testing to pinpoint the specific causative organism.
Eye Cleaning: Continue meticulous eye cleaning procedures as previously outlined.
Antibiotic Treatment: The physician will prescribe appropriate systemic and topical antibiotics based on the results of culture and sensitivity testing. This may involve intravenous antibiotics for severe infections. Penicillin remains a viable option for gonococcal infections, alongside other antibiotics like ceftriaxime or cefotaxime.
Topical Antibiotic Ointments: Utilize Neomycin or tetracycline eye ointment to prevent eyelid adhesion and maintain lubrication.
Medical Management: Purulent discharge in the eyes of the newborn baby.
-> Take history and examine
1. Rx for the baby:
Always wear gloves when handling the infant and their eyes.
Cover the inflamed eye with gauze before opening the eyelids for your own protection.
Clean the eye with saline or water gently to remove discharge.
Apply tetracycline eye ointment hourly for the first 24 hours, then reduce frequency to every 8-hourly for a total of 10 days.
PLUS:
Ceftriaxone 125 mg IM stat. as a single dose.
OR Erythromycin syrup 15 mg/kg body weight 6 hourly x 2/52. administer for 2 weeks.
2. Rx for the mother:
Ceftriaxone 250 mg IM stat. single intramuscular injection.
PLUS: Erythromycin 500 mg for 7 days. oral administration for one week.
3. Rx for partners:
Ciprofloxacin 500 mg stat. as a single oral dose.
Septrin 5 tablets BD x3/7. twice daily for 3 days.
PLUS:
Doxycycline 100 mg BD x7/7. twice daily for one week.
OR Tetracycline 500 mg 6×7/7. six times a day for one week.
Educate on compliance:
Schedule a follow-up return visit to monitor progress.
Provide mother and partner with condoms and offer counseling on risk reduction for future infections.
In case of specific causative organisms:
Gonococcal Ophthalmia Neonatorum:
Infant Isolation: Isolate the infant for the first 24 hours of treatment to minimize transmission risk.
Eye Irrigation: Irrigate the eyes frequently, every 1-2 hours, with sterile isotonic saline until the discharge clears completely.
Systemic Antibiotics: For culture-positive cases or severe infections, systemic antibiotic therapy is crucial. Ceftriaxone (25-50 mg/kg IV or IM) or cefotaxime (100 mg/kg IM or IV) is typically administered as a single dose for localized infection. A 7-day course is recommended for disseminated gonococcal infection.
Chlamydial Ophthalmia Neonatorum:
Oral Erythromycin: Oral erythromycin suspension (40 mg/kg/day divided into four doses) is administered for a full 14 days.
Systemic Therapy Essential: Topical treatment alone is insufficient for chlamydial infections; systemic therapy is critical to prevent systemic spread beyond the eyes.
Herpes Simplex Ophthalmia Neonatorum:
Infant Isolation: The infant requires isolation precautions to prevent viral spread.
Systemic Acyclovir: Systemic acyclovir (20 mg/kg IV every 8 hours IV) for two weeks is the standard treatment regimen.
Topical Antivirals (Adjunctive): Topical therapy with 3% vidarabine or 0.1% iododeoxyuridine ointment (applied five times daily for 10 days) may be added as adjunctive therapy.
Ophthalmological Consultation: Severe cases necessitate prompt and immediate ophthalmological consultation and co-management.
Nursing Care (Maternity Centre and Hospital):
General Hygiene: Maintain meticulous hygiene standards, including frequent handwashing, use of clean linens, and maintaining a clean and sanitary environment.
Eye Care: Continue frequent eye cleaning as previously described to remove discharge and prevent eyelid crusting.
Comfort Measures: Provide comfort measures to reduce the infant’s discomfort, such as gentle swaddling and minimizing bright light.
Frequent Eye Cleaning: Gently cleanse the eyes with sterile saline or sterile water every 2-4 hours, utilizing a separate sterile swab for each eye to prevent cross-contamination.
Medication Administration: Administer topical and systemic medications exactly as prescribed, ensuring correct dosage and frequency of administration.
Monitoring: Closely monitor the infant’s response to treatment, including regular assessment of eyelid swelling, discharge characteristics, and corneal clarity.
Pain Management: Provide comfort measures as needed for pain relief, such as cuddling and soothing techniques.
Education: Educate the parents thoroughly on the importance of adherence to the prescribed treatment regimen, proper eye cleaning techniques, and the necessity for scheduled follow-up appointments.
Complications:
Corneal Ulceration and Scarring: This can result in permanent visual impairment or even blindness if left untreated or if severe.
Perforation of the Cornea: A serious complication that necessitates urgent surgical intervention to repair.
Endophthalmitis: Infection extending to the internal structures of the eye, potentially leading to severe vision loss.
Meningitis: (Rare, but possible, particularly in cases of gonococcal infection). Infection of the membranes surrounding the brain and spinal cord, requiring intensive medical management.
Sepsis: A life-threatening bloodstream infection, demanding immediate and aggressive treatment.

CONJUNCTIVITIS (RED EYE)
Conjunctivitis, commonly known as “pink eye”, is characterized by inflammation of the conjunctiva. This delicate membrane lines the inner eyelid and covers the white part of the eyeball.
Types of Conjunctivitis:
Bacterial Conjunctivitis: This form arises from a bacterial infection. Common culprits include bacteria like Staphylococcus species or Streptococcus species.
Viral Conjunctivitis: Often triggered by viral infections, with adenovirus being a frequent cause. This type is highly contagious.
Allergic Conjunctivitis: An immune response to allergens. Substances like pollen, animal dander, or dust mites, as well as certain cosmetics or medications, can provoke this reaction.
Causes of Conjunctivitis:
Bacterial Agents:
Staphylococcus aureus
Staphylococcus epidermidis
Streptococcus pneumoniae
Haemophilus influenzae
Less frequently, certain sexually transmitted infections (STIs) such as Chlamydia trachomatis and Neisseria gonorrhoeae can also lead to bacterial conjunctivitis.
Viral Agents:
Adenoviruses are a major cause.
Enteroviruses
Herpes simplex virus (HSV)
Herpes zoster ophthalmicus (varicella-zoster virus)
Molluscum contagiosum virus
Measles virus (rubeola)
Mumps virus
Rubella virus (German measles)
Epstein-Barr virus (infectious mononucleosis)
Human Immunodeficiency Virus (HIV)
Allergic Triggers:
Pollen from trees, grasses, and weeds.
Animal dander shed by pets.
Dust mites prevalent in house dust.
Signs and Symptoms of Conjunctivitis:
Bacterial Conjunctivitis Symptoms:
Redness in one or both eyes.
A burning, itchy, or gritty feeling within the eye, sometimes described as mild discomfort.
Increased tear production, resulting in watery eyes.
A thick, sticky discharge, often yellow or greenish, that can cause the eyelids to stick together, especially after sleep.
Swelling of the eyelids.
Sensitivity to bright light may be present, but is usually mild.
Swollen lymph nodes located just in front of the ears may occur.
Viral Conjunctivitis Symptoms:
Pronounced redness of the eye or eyes.
Burning, a sensation of grittiness, or mild pain inside the eye.
Watery discharge is typical, though some mucus may be present.
Crusting of the eyelids can occur, particularly noticeable upon waking.
Swollen and red eyelids.
Increased sensitivity to light.
Swelling of the preauricular lymph nodes (nodes in front of the ears).
Other symptoms of a viral illness, such as a runny nose or sore throat, may accompany viral conjunctivitis.
Allergic Conjunctivitis Symptoms:
Excessive tearing and watery eyes.
Intense itching of the eyes is a hallmark symptom.
Swollen and reddened eyelids and conjunctiva.
Sensitivity to light (photophobia) can occur.
Management of Conjunctivitis:
Bacterial Conjunctivitis Treatment:
Topical antibiotic eye drops or ointments are typically prescribed. Chloramphenicol or gentamicin eye drops are commonly used, initially applied frequently (e.g., every 2-3 hours for the first couple of days), then reduced in frequency.
Treatment adjustments may be needed based on bacterial culture and sensitivity testing, especially in severe or persistent cases.
Conjunctivitis caused by Neisseria gonorrhoeae requires urgent and aggressive treatment as per STI management protocols.
Steroid eye drops should be used with caution and for limited durations only, as advised by a healthcare professional.
Mild cases might resolve on their own within a week or two without specific medication.
Regularly clean any discharge from the eye area using a clean, soft cloth, sterile gauze, or cotton ball moistened with water.
Artificial tears (lubricating eye drops) can provide comfort. Avoid contact lens wear until the infection is completely resolved.
Viral Conjunctivitis Treatment:
For most cases, specific antiviral treatment is not necessary. Reassurance and symptomatic relief are usually sufficient.
In certain severe cases, particularly those caused by herpes viruses, antiviral medications might be considered. Systemic corticosteroids like oral prednisolone might be used in rare, severe cases under specialist guidance.
Cool or warm compresses applied to the eye can help soothe discomfort. Gentle cleaning of discharge with warm water is recommended. Lubricating eye drops can alleviate dryness and irritation.
It is essential to avoid wearing contact lenses until the viral infection clears up.
Allergic Conjunctivitis Treatment:
Cold compresses applied to the eyes can provide relief from itching and swelling.
Topical steroid eye drops might be prescribed for persistent or severe allergic conjunctivitis, but generally for short-term use only, due to potential side effects.
Maintaining good facial and eyelid hygiene can help reduce allergen exposure.
Antihistamine eye drops or oral antihistamines can help control itching and allergic symptoms. In some cases, mast cell stabilizer eye drops may be used for longer-term management. Betamethasone or hydrocortisone eye drops may be prescribed to be used frequently initially (e.g., every 1-2 hours until inflammation is controlled) and then tapered to twice daily.
We are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved