Obstetric Anatomy and Physiology
Moulding of the Fetal Skull
Table of Contents
MOULDING OF THE FETAL SKULL
Definition
This is the change of size and shape of the fetal skull, made possible by sutures and fontanelles, during labor. This change allows the skull to reduce its engaging diameters in order to fit into the pelvis.
Moulding is only possible when the head is presenting at the pelvic brim. Moulding is the result of compression of the engaging diameter and elongation of those which are not engaged.
How Moulding Takes Place
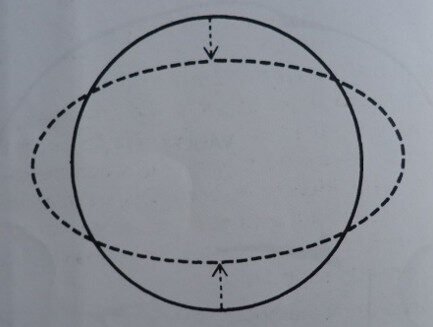
Demonstration of the principle of moulding: the diameter compressed is diminished; the diameter at right angles with it is elongated.
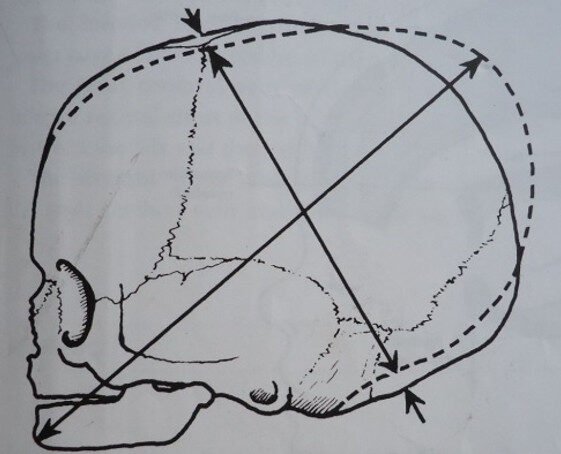
When the fetal head is subjected to pressure, it causes the bones of the vault to overlap at the suture lines as follows:
The parietal bones overlap each other.
The frontal and occipital bones slide under the parietal bones.
This reduces the diameter, making it easier for the head to pass through the birth canal (by compressing the engaging diameter, reducing it by approximately 1.25 cm).
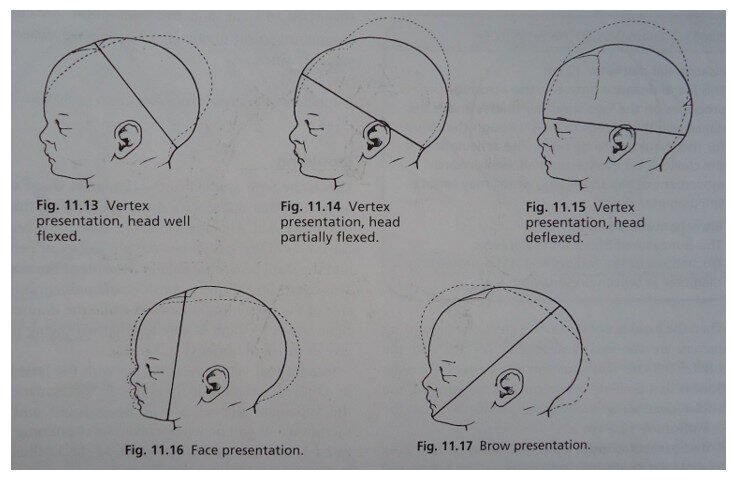
Normal Moulding / Normal Vertex Presentation
Moulding in a normal vertex presentation occurs with the head well-flexed. The suboccipitobregmatic diameter is reduced, and the mentovertical diameter is elongated.
The head is well flexed. This is harmless to the baby, and the moulding disappears after 1-2 days.
Moulding in Various Presentations
Occipito-Posterior Position (OPP) (Abnormal Moulding)
The head is not well-flexed. The occipito-frontal diameter is compressed or reduced. The submentobregmatic diameter is raised. This moulding is known as sugar loaf moulding (Face to pubis).
NB: Caput is on the anterior aspect of the parietal bones.
Face Presentation
The head is completely extended. The submentobregmatic diameter is decreased, and the occipito-frontal diameter is increased. This moulding is known as backward moulding.
NB: Caput is on the face.
Brow Presentation
The head is slightly or partially extended.
The mentovertical diameter is decreased.
The suboccipitobregmatic diameter is increased.
NB: Caput is on the sinciput.
Due to poor moulding, the two membranes may rupture, causing bleeding: (1) Falx cerebri (separates the two halves of the cerebrum) and (2) Tentorium cerebri (separates the cerebrum and cerebellum).
Table: Relationship of Head Attitude, Presentation, and Engaging Diameters
Attitude of the head | Presentation | Engaging diameter and length | Extent of the engaging diameter |
|---|---|---|---|
1. Complete flexion | Vertex | Suboccipitobregmatic
Length: 9.5cm, distends the perineum during labor | Estimated from below the occipital protuberance to the mid-point of the Bregma |
2. Poorly flexed or deflexed head | Vertex (occipitoposterior) position | Suboccipitofrontal
Length: 10cm | From below the occipital protuberance to the center of the frontal suture |
3. Head in the military attitude | Cephalic (crown presentation) occipitoposterior | Occipitofrontal
Length: 11.5cm | From the occipital protuberance to the mid-point of the frontal suture |
4. Head partially extended | Brow | Mentovertical
Length: 13.5cm
– may result in obstructed labor | From the chin to the highest point on the vertex |
5. Head fully extended | Face | Submentobregmatic
Length: 9.5cm
Submentovertical
Length: 11.5cm | From where the chin joins the neck to the Bregma
From where the chin joins the neck to the highest point on the vertex |
Abnormal, Excessive, and Rapid Moulding
Terms Used in Abnormal Moulding
Any moulding not from a normal vertex presentation is considered to be abnormal. Abnormal or severe moulding may cause cerebral injury or cerebral hemorrhage.
Excessive Moulding is Caused By:
Large engaging diameters.
Contracted pelvis or obstructed labor.
Face presentation (bones of the face do not mould).
Large baby.
Rigid pelvic floor resistance to the fetal head.
Occipito-posterior position.
Prematurity (in cases of a big premature baby).
Rapid Moulding is Caused By:
After-coming head in breech delivery.
Persistent Occipito-Posterior (POP) or “face to pubis” (pull of Falx cerebri, tear of Tentorium).
Brow presentation.
(1) A precipitate labor.
(2) 2nd twin delivery.
A baby born with excessive moulding should be continuously nursed for at least the first 24 hours of life, observing for signs of cerebral damage and irritation.
Complications of Abnormal / Excessive Moulding
Caput succedaneum
Mental retardation
Brain damage
Intracranial damage
Perineal, cervical, or uterine tears
Vesicovaginal fistula, Rectovaginal fistula
Puerperal sepsis
Postpartum hemorrhage
Prolonged labor, obstructed labor
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowWe are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved