Obstetric Anatomy and Physiology
The Breasts
Table of Contents
Anatomy and Structure
Definition and Situation
The breasts, or mammary glands, are glandular tissues and accessory organs of reproduction. They are two in number, situated on either side of the sternum, extending vertically from the 2nd rib up to the 6th rib. They are embedded in the superficial fascia of the chest wall, overlying the Pectoralis Major muscle, and are stabilized by suspensory ligaments.
Shape and Size
The shape and size of the breast vary significantly based on an individual’s stage of development, overall body size, and age.
Tail of Spence (Axillary Tail): A tail of glandular tissue extends toward the axilla (armpit). Its primary function is to stabilize the breast.
Gross Structure
Component | Description |
|---|---|
Skin | The outermost covering, providing protection for the internal structures. |
Areola | A circular, 2.5 cm diameter area of loose, pigmented skin found in the center of each breast. It darkens during pregnancy due to Melanin in preparation for lactation. |
Montgomery’s Tubercles | 18–20 sebaceous glands situated around the nipple, within the areola. They produce Sebum to lubricate the nipple, keeping it smooth and pliable. During pregnancy, these glands enlarge and become more prominent. |
Nipple | A 6mm-long protuberance lying in the center of the areola, typically at the level of the 4th rib. It is composed of pigmented, erectile tissue. Its surface is perforated by small orifices, or milk jets, which are the openings of the lactiferous ducts. The nipple is a highly sensitive structure. |
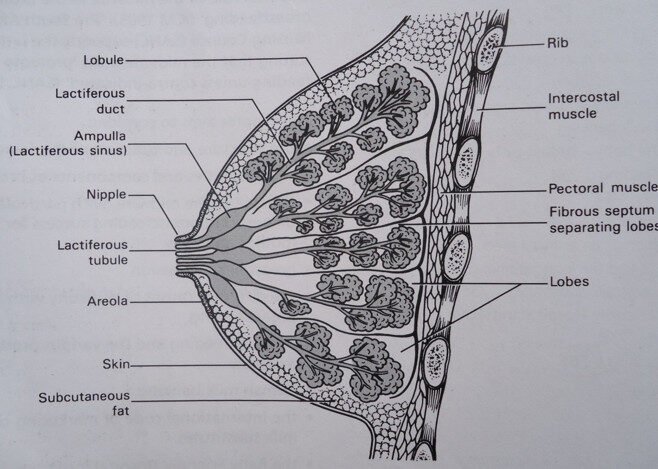
Microscopic Structure
The breast has an internal structure resembling a “cut orange.” It is mainly composed of glandular tissues surrounded by a pad of fatty tissue beneath the skin. The glandular tissue is divided into 18–20 lobes by fibrous tissue, with each lobe functioning as a self-contained unit.
Each lobe is composed of the following parts, arranged for milk secretion and transport:
Alveoli / Acini Cells: These are the milk-secreting cells.
Lactiferous Tubules: Small ducts that connect the alveoli to the main lactiferous ducts, into which they empty their milk.
Lactiferous Ducts: Central ducts that receive milk from the tubules and connect to the Ampulla.
Ampulla (Milk Reservoirs): A widened portion of the main duct where milk is temporarily stored before consumption.
Milk Jets: The continuation of the lactiferous ducts extending from the Ampulla and opening at the surface of the nipple.
Blood, Lymph, and Nerve Supply
Blood Supply: Blood is supplied by the Internal Mammary Artery (a branch of the subclavian artery), the External Mammary Artery (a branch of the thoracic artery), and the Intercostal Arteries passing through the intercostal spaces.
Venous Return: Blood is returned through corresponding vessels into the Internal Mammary and Axillary Veins.
Lymphatic Drainage: Lymph drains primarily into the Axillary Glands, the glands of the medial sternum, and into the portal fissures of the liver. The lymphatic vessels of each breast communicate with one another.
Nerve Supply: The activity of the glandular tissue is controlled by hormones. The overlying skin is supplied by branches of the thoracic nerves. There is sympathetic nerve supply, particularly around the areola and nipple, which contributes to its sensitivity.
Functions
The primary function of the breast is to produce and supply milk to the infant.
THE MICROSCOPIC STURCTURE OF THE FEMALE BREAST
II. Changes During Pregnancy
Changes in the breast during pregnancy are induced by hormones produced by the placenta and corpus luteum (or ovarian hormones).
Hormonal Influence
Hormone | Effect |
|---|---|
Oestrogen and H.C.G. | Stimulates the growth of glandular tissue and ducts, increases adipose (fatty) tissue, and strengthens fibrous tissue. |
Progesterone | Activates the Acini Cells to produce milk. |
Melanin | Responsible for the darkening of the primary areola and the formation of the secondary areola. |
These hormones are present in the bloodstream throughout pregnancy. After delivery, they are withdrawn, and Prolactin takes over.
Timeline of Physical Changes
The changes in the breast are typically experienced by the mother as early as 3 weeks of pregnancy:
3rd – 4th Weeks: Breasts become nodular and tender to the touch. A prickling, tingling sensation is experienced due to increased blood supply and tissue growth.
6th Week: Marked enlargement of the breast.
8th Week: Superficial veins become visible due to increased blood supply.
8th Week (Glands): The sebaceous glands (Montgomery’s tubercles) enlarge and secrete an oily substance to lubricate the nipple in preparation for breastfeeding.
12th Week: Fluid is present in the breast, and there is marked darkening of the primary areola.
16th Week: Colostrum (a clear, straw-coloured fluid) can be expressed or secreted.
Function of Colostrum at this stage: To clear the lactiferous ducts and tubules of dead epithelial tissue, preparing for the free flow of milk.
Secondary Areola: Appears as a mottled area of pigmentation extending beyond the primary areola, sometimes covering half the breast. This pigmentation may persist for up to 12 months post-delivery.
Note: The midwife must reassure the mother that any pain accompanying these changes is normal.
III. Importance of Breast Knowledge to a Midwife
The midwife’s knowledge of the breast is crucial for ensuring successful maternal-infant health outcomes:
Preparation for Lactation: Enables the midwife to teach the mother proper breast care, including wearing a well-fitting bra with wide straps for support, and advising on techniques (pulling and rolling) for flat or inverted nipples.
Detection and Management of Abnormalities: Facilitates the early detection and prompt management of breast abnormalities or infections during examination.
Health Education: Allows the midwife to advise the mother accurately on the expected breast changes during pregnancy, the puerperium, or before pregnancy.
Emphasis on Key Care Points: Helps the midwife emphasize crucial points in health education, such as breast hygiene, nipple preparation, and the importance of self-palpation to exclude hard lumps.
Pregnancy Detection: Knowledge of breast changes and their onset time can help the midwife detect or confirm a pregnancy.
Gestation Estimation: In cases where the mother is unsure, knowledge of the timeline of breast changes can help the midwife estimate the gestational age.
Proper Fixation: Enables the midwife to teach the mother the correct positioning and proper fixation of the baby during breastfeeding, ensuring the baby sucks over the Ampulla area.
IV. Stages of Breast Development
At Birth
Breast tissue is present but confined to the nipple area, which is prominent. Sometimes, in the first few days of life, breast tissue may enlarge and secrete fluid (“witch’s milk”) due to the action of circulating maternal hormones in the infant’s bloodstream. This condition requires no treatment and subsides as hormonal levels adjust.
At Puberty
Hormone levels begin to alter, usually before the onset of menstruation. The breasts slowly begin to develop:
Glandular tissues, lactiferous tubules, and ducts continue to proliferate.
The amount of fatty and fibrous tissue increases.
The nipple and areola become more pronounced.
Child-Bearing Age
In the latter half of the menstrual cycle, many women complain of breast changes (e.g., tenderness, fullness) similar to those in early pregnancy. These are caused by Progesterone produced by the corpus luteum and disappear with the onset of menstrual flow as progesterone levels decrease.
After Delivery
The breast is considered to have reached full development on the 1st to 3rd day after delivery, when it is capable of full milk secretion.
Following the delivery of the placenta, the levels of Oestrogen and Progesterone gradually reduce.
Around the 3rd day, the Anterior Pituitary Gland releases Prolactin, and the Posterior Pituitary Gland releases Oxytocin, initiating true lactation.
V. Colostrum
Colostrum is a clear, straw-coloured fluid present in the breast from 32 weeks of pregnancy onwards until the end of the 3rd day of the puerperium.
Composition
Colostrum is highly nutritious despite its small volume:
Proteins ($\approx 8\%$)
Leucocytes (White blood cells)
Mineral salts
Colostrum corpuscles
Fats
Lactose
Dead epithelial cast
Functions
Clearing Ducts: Keeps the lactiferous ducts and tubules clear.
Laxative Effect: Acts as a laxative for the infant, helping it to pass its bowels of Meconium.
Nutrition: The high protein content allows for adequate nutrition in the newborn.
Note: The vast majority of newborns do not require complementary feeds of cow’s milk, although some may require extra fluid (boiled water) in the first 48 hours of life.
VI. Physiology of Lactation
Hormonal Control
When the placenta is expelled, the reduction in Oestrogen and Progesterone levels triggers the release of Prolactin from the Anterior Pituitary Gland.
Oestrogen suppresses the action of Prolactin; therefore, milk typically does not “come in” until about the 3rd day post-delivery when Oestrogen levels drop.
Production of Milk
Milk production (formation) relies on an increased blood supply to the breast.
Essential substances (fatty globules and protein molecules) are extracted from the blood within the base of the secreting cells.
These components distend the Alveoli (Acini cells) and push their way through, depending on both the fine adjustment of hormones and good blood circulation.
Passage of Milk (Let-down Reflex)
Two factors are involved in the transit of milk from the secreting cells to the nipple:
Back Pressure: The force of new globules forming in the cells pushes the foremost milk into the lactiferous tubules, then into the lactiferous ducts.
Neuro-Hormonal Reflex:
When the baby is put to suck, the emptying of the Ampulla and large ducts causes them to contract, forcing milk toward the nipple.
Stimulation of the nipple by the sucking baby causes a nervous reflex action.
This reflex causes the Posterior Pituitary Gland (P.P.G.) to directly liberate Oxytocin.
Oxytocin causes further contraction of the ducts and myoepithelial cells, leading to the milk ejection (let-down) reflex.
NB: This same Oxytocin also helps in the contraction of the uterine muscles, aiding in the Involution of the Uterus during the puerperium.
Maintenance of Milk Supply
Milk supply is maintained in response to demand; the more the baby sucks, the better the milk supply. If the baby is not put to the breast, the milk supply fails.
Two factors are responsible for maintenance:
Stimulus: The stimulus of the baby’s gums on the breast, with the suction force applied to the skin of the areola, maintains the neuro-hormonal reflex. If the infant cannot suck, stimulation must be done by emptying the breast by hand.
Complete Emptying: After each feed, the mother must be taught to express any remaining milk by hand if the baby does not finish it all. This ensures a constant, fresh flow of milk and prevents stasis.
VII. Preparation for Successful Lactation
A. During Antenatal Care (A.N.C)
Encourage frequent A.N.C attendance for health education.
Perform proper history-taking and breast examination to detect abnormalities and infections, providing immediate advice, treatment, and screening for delivery location.
Stress Hygiene and Care of the Breast: Advise wearing a supporting brazier with wide straps, and washing the breasts daily with soap and water.
Advise on a good, nourishing diet with plenty of fluids.
Correct any conditions that interfere with lactation (e.g., Anemia).
Preparation of the Nipple: Advise pulling and rolling the nipple between the fingers and thumb after bathing. Dry them with a rough towel to toughen them. For flat nipples, advise the use of nipple shells to create suction and pull the nipple out (as recommended by the late Dr. Waller of Woolwich).
Teach mothers to self-palpate their breasts and report any lumps.
B. During Labour
Proper Management of Labour: Prevent prolonged and obstructed labour, maternal/fetal distress, as these can negatively affect lactation.
Provide Plenty of Fluids to prevent dehydration.
Careful Delivery Management: Prevent excessive perineal tears and trauma to the baby, which can cause psychological effects on the mother and lead to poor lactation due to pain.
Infection Prevention: Use minimal vaginal examinations and aseptic procedures. Keep the bed dry to prevent infection, especially with early membrane rupture.
Ensure frequent emptying of the bladder to prevent prolonged labour and Vesico-Vaginal Fistula (V.V.F.).
Conduct delivery in a clean environment using sterile instruments.
Prevent Post-Partum Hemorrhage in the 2nd and 3rd stages, as resulting Anemia impedes good lactation.
Initiate Breastfeeding: The baby should be fixed on the breast soon after delivery, provided the condition of both mother and baby allows.
Ensure complete expulsion of the placenta and membranes to prevent puerperal sepsis.
C. During Puerperium
Psychological Support: Reassure nervous mothers and encourage them to breastfeed. Ensure she is free of worries.
Provide proper education and supervision in breast management and care.
Ensure the mother gets enough rest and sleep and wears a well-fitting bra. A loose bra can lead to engorged breasts (Engorgement).
Advise on a good, nourishing diet with extra vitamins, iron, and adequate fluids.
Teach the mother how to fix the baby on the breast correctly and how to remove it gently.
Ensure both mother and baby are in a comfortable position during feeding.
Advise the mother not to allow the baby to spend too long on the breast or fall asleep while feeding.
The mother should support the breast tissue away from the baby’s nose to ensure free breathing.
Prevent any condition that interferes with breastfeeding (e.g., swabbing a baby with discharging eyes clean before feeding to prevent breast infection).
Teach the mother to manually express any remaining milk if the breasts are not fully emptied, which prevents engorgement and ensures a constant flow of milk.
NB: The midwife must perform a careful examination of the breast daily
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowWe are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved