Obstetric Anatomy and Physiology
The Female Pelvis
Table of Contents
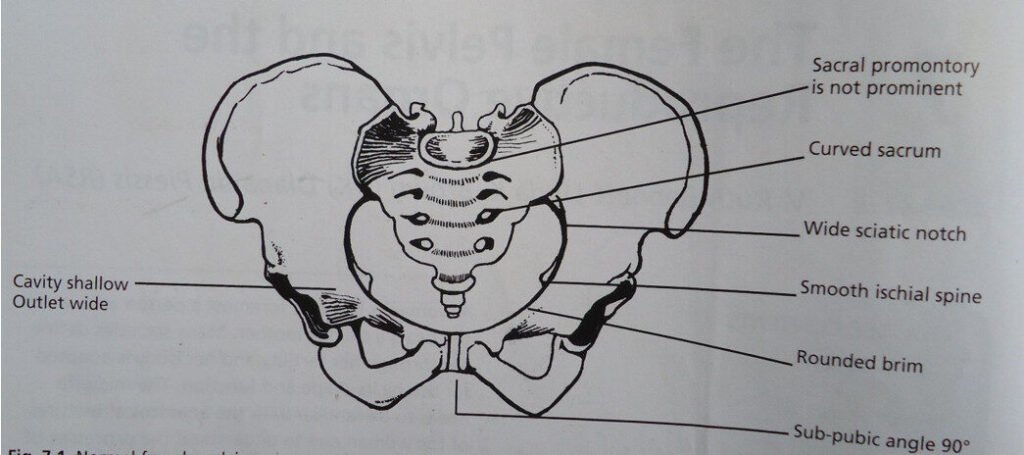
THE NORMAL FEMALE PELVIS
DEFINITION: This is a bony canal through which the fetus must pass in order to be born during the process of birth.
SITUATION: It’s found at the lower end of the spinal cord. The pelvis articulates with the fifth lumbar vertebra above, and the head of each femur in the right and left acetabulum. The weight of the trunk is therefore transmitted through the pelvis to the legs.
SHAPE: It is similar to that of a bony basin. It contains and protects the pelvic organs.
SIZE: It is the largest bone formation in the body.
GROSS STRUCTURE OF THE PELVIS
The pelvis is composed of 4 bones namely:
- 2 innominate bones (hip bones)
- Sacrum
- Coccyx
INNOMINATE BONE
Forms the sides and the front walls of the pelvis. Each innominate bone consists of 3 parts which unite at the acetabulum.
These parts are ilium, ischium, and pubis. Before the age of 25 years these bones are not completely united.
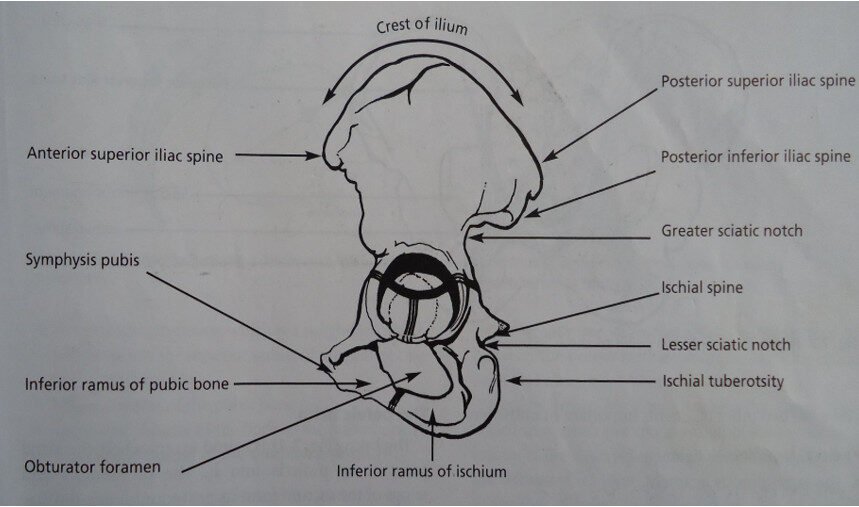
ILIUM:
This is the upper largest (flared) out part which articulates with the ala of the sacrum. It forms the upper 2/5 of the acetabulum. It has 3 parts namely: iliac fossa, iliac crest, iliopectineal line.
- ILIAC FOSSA: This is the inner aspect of the ilium. It’s smooth and concave. But the outer side is rough which gives the attachment of muscles to the buttocks.
- ILIOPECTINEAL LINE: This is a ridge lined below the iliac fossa, which terminates anteriorly in a bony prominence called iliopectineal eminence.
- ILIAC CREST: This is the upper border of the ilium; anteriorly the iliac crest terminates at the bony prominence known as anterior superior iliac spine. (A short distance 2.5 cm) – Below is the anterior inferior iliac spine. Posteriorly the iliac crest ends at another part posterior superior iliac spine and posterior inferior iliac spine below and the upper border of greater sciatic notch through which sciatic nerve passes.
THE ISCHIUM (BONE OF SEAT):
This is the thick lower part of the innominate bone. It forms the 2/5 of the acetabulum and has 2 parts i.e. ischial tuberosity and ischial spine.
- ISCHIAL TUBEROSITY:
It’s a large prominent (the body of ischium) and it’s a point of the ischial tuberosity that the body rests on sitting. About 2.5 cm above the tuberosity, the upward projection called ischial spine, which divides the greater and lesser sciatic notches. NB: In labor the station of the fetal head is estimated in relation to the ischial spine.
PUBIS:
It covers the remaining 1/5 of the acetabulum. This forms the anterior part of the pelvis. Each of the pubic bones has a body and 2 rami. The ramus joins the ilium at a thick point called the iliopectineal eminence. The descending ramus forms part of the obturator foramen.
The body of the pubic bone articulates at the symphysis pubis by a pad of cartilage between them.
SACRUM:
This is a wedge-shaped bone which forms the back of the pelvis. It is made up of five fused vertebrae. The anterior surface of sacrum is concave and posterior is convex. The cavity is called the hollow of the sacrum. The upper border of the sacral vertebra juts/protrudes towards and (hangs) projects over the hollow of the sacrum; it is called the sacral promontory.,
The first sacral vertebra articulates with the 5th lumbar vertebra at the lumbosacral joint. The lateral masses of bones, on either side of the 1st sacral vertebra are the ala or wings of the sacrum and they articulate with the ilium at the sacroiliac joint. The four foramina on each side of the sacrum are for the passage of lymphatic nerves and blood vessels.
The small canal on the posterior aspect of the sacrum is called the sacral canal, which opens at a level of 5th sacral vertebra. At the level of the 2nd and 3rd sacral vertebrae the nerves spread out to form the cauda equina, to supply the pelvic organs. The posterior is rough to form the attachment of muscles.
COCCYX:
Is made up of 4 (four) fused coccygeal vertebrae; it’s triangular in shape with the base lying in the uppermost and articulates with the sacrum at sacrococcygeal joint. During delivery it tilts backward to allow passage of the baby.
THE PELVIC JOINTS
- Two sacroiliac joints: These lie between the bodies of the first two sacral vertebrae and the upper surface of the ilium. They are slightly movable joints and are surrounded and separated by ligaments.
- Symphysis pubis: This is formed by the pubic bones which are united by a pad of cartilage. It’s almost 4 cm in length and has a support ligament around it. During later months of pregnancy it widens and a degree of some movement may give rise to pain when walking.
- Sacrococcygeal joint: This is formed by the articulation of the base of the coccyx and the tip of the sacrum above, and allows the coccyx to bend backwards, during labor allows more room for the fetal head during passage through the birth canal.
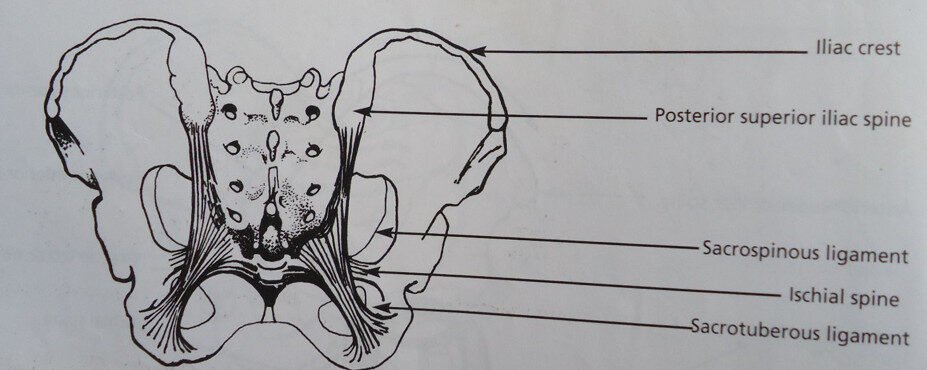
PELVIC LIGAMENTS .
Posterior view of the pelvis to show ligaments.
Each pelvic joint is held together by ligament e.g. interpubic ligament at the symphysis pubis.
- SACROILIAC LIGAMENTS: This strengthens the sacroiliac joints. They are two in number. They are the strongest in the body.
- SACROCOCCYGEAL LIGAMENT: These surround the sacrococcygeal joint.
OTHER LIGAMENTS IMPORTANT IN MIDWIFERY ARE
(1) The sacrotuberous ligament: These are two; they stretch from the lower border of the sacrum to the ischial tuberosities.
(2) Sacrospinous ligament: They are two in number running beneath the sacrotuberous ligament, extends from the lower border of the sacrum to the ischial spines.
Other ligaments found on the pelvis are:
(1) 2 Poupart’s ligament or (inguinal ligament): This extends between the anterior superior iliac spines to the body of the pubis.
(2) 2 Lacunar ligaments: Stretches from the iliopectineal eminence to the bodies of the pubic bone. Each lies under the inguinal ligaments.
(3) 2 Obturator membranes: Fills the obturator foramen.
THE FUNCTIONS OF THE PELVIS
- It is a passage through which a fetus or a baby must pass in order to be born.
- It contains and protects the internal reproductive organs.
- It transmits the weight of the trunk to legs thus connects the spine to the lower limbs.
- It is for attachment of muscles of (buttocks) gluteal muscles.
- It helps us to sit and move.
DIVISION OF THE PELVIS
The pelvis is divided into two parts: i.e.
(i) The false and
(ii) the true pelvis
THE FALSE PELVIS/GREATER PELVIS/MAJOR PELVIS
Lies above the pelvic brim and is of less importance in midwifery.
THE TRUE PELVIS/LESSER PELVIS/PELVIS MINOR
Includes the pelvic brim and all the bones that lie below it, it has the brim, cavity and outlet and forms a curved canal through which the fetus must pass to be born.
THE LANDMARKS OF THE TRUE PELVIS
(1) Sacral promontory
(2) The hollow of the sacrum
(3) Ischial tuberosities
(4) Ischial spines
(5) Subpubic arch
THE PELVIC BRIM (INLET)
Definition: It is a ridge of bones which separates the true pelvis from the false pelvis.
SHAPE: It is almost round in shape except where the sacral promontory protrudes inwards. It is important in midwifery because it’s where the fetal head engages first.
CIRCUMFERENCE: It is 36 cm compared to the head which is 34.5 cm.
BOUNDARIES OF THE BRIM
- (a) Sacral promontory
- (b) Ala of the sacrum (wing)
- (c) Sacroiliac joint
- (d) Iliopectineal line
- (e) Iliopectineal eminence
- (f) Inner border of the superior pubic ramus
- (g) Body of the pubic bone
- (h) The upper inner border of the symphysis pubis
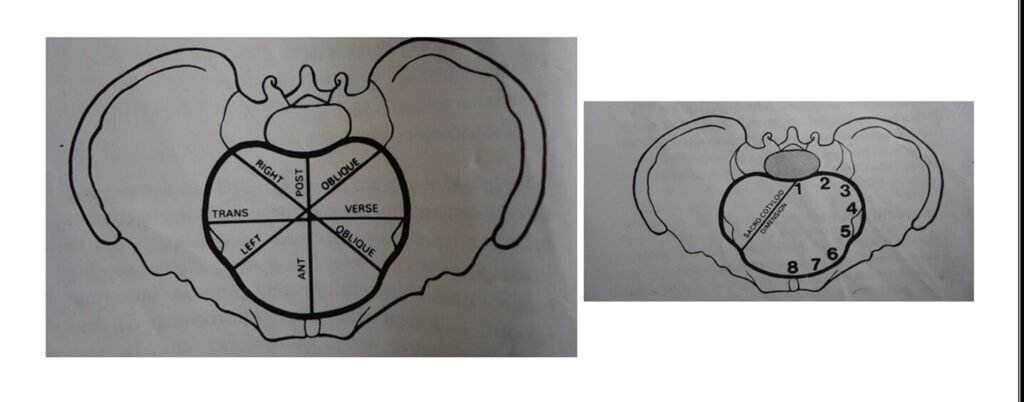
THE DIAMETERS OF THE BRIM (MEASUREMENTS)
- The anteroposterior diameter: Measured from the sacral promontory to the upper inner border of the symphysis pubis about 1.25 cm from the center. It is equal to 11 cm.
- Oblique diameter: Measured from one sacroiliac joint to the iliopectineal eminence on the opposite side and measures 12 cm. They are two oblique diameters (left and right).
- The transverse diameter: It is the largest of the three and it is measured from the iliopectineal line to the other side and measures 13 cm.
- Sacro-cotyloid diameter: It is measured from the sacral promontory to the iliopectineal eminence on each side and measures 9.5 cm.
DIAGRAM SHOWING THE DIAMETERS OF THE BRIM
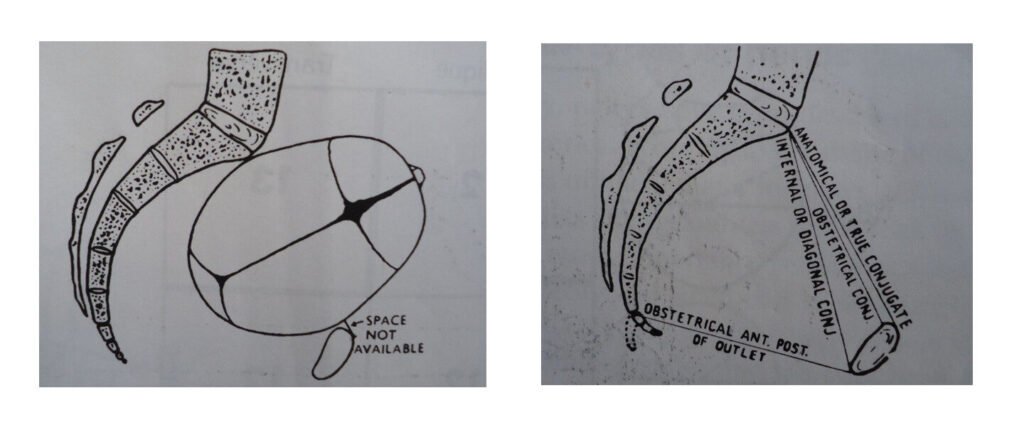
OTHER MEASUREMENTS OF THE ANTEROPOSTERIOR DIAMETERS/CONJUGATES
These are 3 diameters measured from front to back extending from the sacral promontory to the symphysis pubis.
- The anatomical diameter/conjugate: It is taken from the sacral promontory to the uppermost point of the symphysis pubis and it measures 12 cm.
- The obstetrical conjugate: It’s taken from the sacral promontory to the posterior border of the upper symphysis pubis/upper inner border of the symphysis pubis which is about 1.25 cm lower and measures 11 cm. Fetal head negotiating the narrow obstetrical conjugate. The reason for this is that the obstetrical conjugate represents the available space for the passage of the fetus. The term true conjugate may be used for both terms.
- Diagonal conjugate/internal diameter: Is also measured anteroposteriorly from the lower border of the symphysis pubis to the sacral promontory. Done during vaginal examination as pelvic assessment measures 12 to 13 cm.
IMPORTANT LANDMARKS OF THE BRIM
- Sacral promontory: If prominent, reduces the anteroposterior diameter thus obstructed labor.
- Iliopectineal eminence: It is important because this is the point where the denominator faces to determine position.
- Symphysis pubis: If narrow, it reduces the anteroposterior diameter.
- The oblique diameter: It is important for the engagement of the fetal head.
THE PELVIC CAVITY
DEFINITION:
The cavity extends from the brim above to the outlet below.
SIZE: The anterior wall is formed by the pubic bone and symphysis pubis which measures 4 cm. The posterior wall is formed by the curve of the sacrum which is about 12 cm long. Its lateral walls are the sides of the pelvis because of difference in measurement of cavity from the curved canal.
SHAPE: The lateral walls formed (the cavity is circular in shape) by imaginary lines drawn across.
BOUNDARIES OF THE CAVITY
- Posteriorly: Hollow of the sacrum and measures about 11 cm.
- Anteriorly: It is formed by the symphysis pubis and it is equal to 4 cm.
- Laterally: The greater sciatic notch, the back of the acetabulum, the obturator foramen, the back of the body of the pubic bone.
DIAMETERS/MEASUREMENTS OF THE CAVITY
The cavity is circular in shape and all diameters measure 12 cm.
- The anteroposterior diameter: It is taken from the junction of the 2nd and 3rd sacral vertebrae to the midpoint of the symphysis pubis.
- The oblique diameter: It runs parallel to the oblique diameter of the pelvic brim. There are no fixed points to measure between the two diameters.
- The transverse diameter: It is measured between the points furthest apart, on the lateral pelvic walls.
IMPORTANT LANDMARKS OF THE CAVITY
- Hollow of the sacrum: This is a curve found in the sacrum and it allows good rotation of the fetal head, it should be well curved.
- The greater sciatic notch: Should be circular in shape and wide to allow free rotation of the fetal head.
- Symphysis pubis: Should not be narrow, it should be wide to allow the baby to pass through the pelvis.
PELVIC OUTLET This is the lowest part of the true pelvis.
SHAPE: It is diamond shaped.
CIRCUMFERENCE: It is 36 cm.
Two outlets are described as:
(a) Anatomical outlet
(b) Obstetrical outlet
ANATOMICAL OUTLET (BOUNDARIES)
- The tip of the coccyx
- Sacrotuberous ligament (posteriorly)
- Ischial tuberosities (laterally)
- The pubic arch and
- The lower border of the symphysis pubis
- Inferior pubic ramus
OBSTETRICAL OUTLET
Is more important in midwifery because it includes the narrow pelvic space through which the fetus must pass. These are all fixed points and useful landmarks for taking pelvic assessment and because the coccyx can tilt backwards and the ligaments are capable of stretching. There is more room for the fetus to pass than it first appears. The available room is known as the obstetrical outlet.
BOUNDARIES OF THE OBSTETRICAL OUTLET
(1) The lower border of the symphysis pubis
(2) Ischial spines
(3) Sacrospinous ligament
(4) Lower border of the sacrum
THE LANDMARKS OF THE OUTLET
(1) Ischial tuberosities should accommodate 4 knuckles
(2) Anteroposterior diameter where the internal rotation of the shoulder takes place
(3) Ischial spines: If prominent it reduces the transverse diameter
(4) The tip of the coccyx tilts backwards during labor
THE DIAMETERS OF THE OUTLET
- Anteroposterior: 13 cm
- Oblique: 12 cm
- Transverse: 11 cm
THE OUTLET: Is diamond shaped and its diameters are:
(i) ANTEROPOSTERIOR DIAMETER: It is measured from the lower border of the symphysis pubis to the sacrococcygeal joint. It measures 13 cm; the coccyx can tilt backwards during labor. This diameter includes the space available during delivery.
(ii) OBLIQUE DIAMETER: It is measured between the obturator foramen and sacrospinous ligament although there is no fixed measurement 12 cm.
(iii) TRANSVERSE DIAMETER: Is measured between the two ischial spines and measures 11 cm. It is the narrowest diameter in the pelvic outlet.
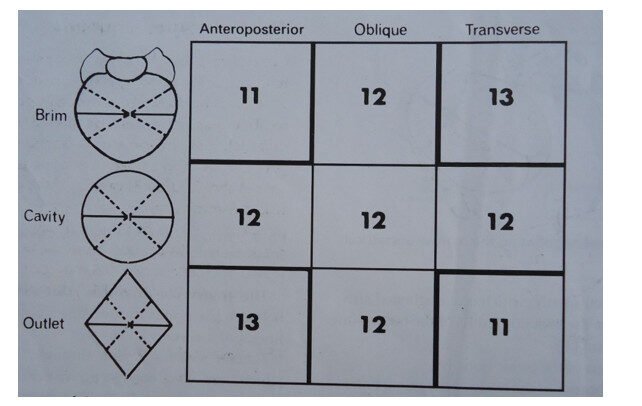
MEASUREMENTS OF THE PELVIC CANAL IN CENTIMETRES
| PELVIS | AP | OB | TR |
|---|---|---|---|
| Brim | 11 cm | 12 cm | 13 cm |
| Cavity | 12 cm | 12 cm | 12 cm |
| Outlet | 13 cm | 12 cm | 11 cm |
SUMMARY OF THE MEASUREMENTS OF THE DIAMETERS OF THE BRIM, CAVITY AND OUTLET.
NOTE THE PELVIC DIAMETERS
The brim, cavity and outlet are all shaped in a way that their diameters can be estimated and used to identify the route taken by the fetus as it negotiates the pelvis. With knowledge of presentation, position and attitude of the fetus, this information enables a midwife to:
- To identify whether there is sufficient room for the passage of the fetus.
- To understand why the fetus rotates as it moves through the pelvis, accommodating to spaces and prominent landmarks it encounters.
PLANES OF THE PELVIS
These are imaginary flat surfaces drawn at the level of the brim cavity and outlet.
(1) When the person is standing upright, the angle of the brim is 60° with the floor.
(2) The angle of the plane of the cavity with the floor is 30°.
(3) The angle of the plane of the outlet with the floor is 15°.
DIAGRAM OF THE PLANE OF THE PELVIS
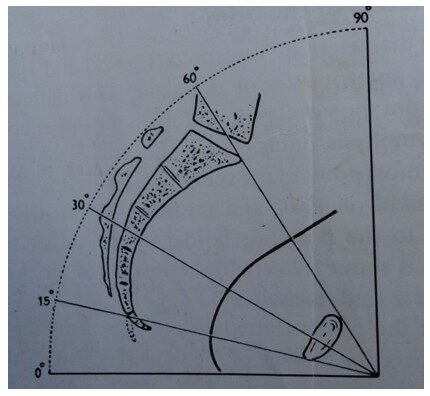
Median section of the pelvis showing the inclination of the planes and axis of the pelvic canal.
Fetal head entering plane of pelvic brim and leaving plane of outlet.
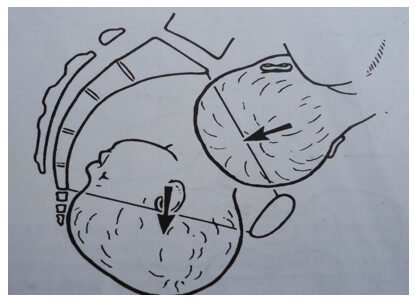
CURVE OF CARUS
Is a line drawn exactly halfway between the anterior and posterior wall at right angles to each of the planes and is said to be the path which the fetus takes as it travels through the birth canal.
SIGNIFICANCE OF THE KNOWLEDGE OF THE FEMALE PELVIS
(1) Assessment of weeks of gestation: In early pregnancy at 12 weeks the uterus rises out of the pelvis from now onwards, during pregnancy the height of fundus is assessed from the symphysis pubis.
(2) Give of the pelvic joints and softening of ligaments: This knowledge helps the midwife to understand some minor disorders like backache and lower abdominal pain and she can give correct advice about rest, position and exercise.
(3) Size and shape: Knowing the normal shape and size, she can recognize deviation from normal by head fitting at 36 weeks when the head is big enough to be compared with a pelvic brim and internal pelvic assessment. She can recognize deviation such as reduction of size in the anteroposterior (AP) diameter, straight hollow of the sacrum, prominent ischial spine, narrow subpubic arch or outlet. This helps her to recognize its disproportion and when to expect complication or difficult deliveries.
(4) Progress of labor: This she can assess by descent of the presenting part in the pelvis or on abdominal examination and on vaginal examination when not in relation with ischial spines. She will know if the head is high and not yet engaged or in mid cavity. When the head is engaged normal delivery can be expected (can recognize abnormalities e.g. transverse lie).
(5) Curve of birth canal: Her knowledge of the birth canal helps her to deliver the head according to the shape allowing the smallest diameter to distend the perineum and easier delivery.
(6) Fundal pressure and controlled cord traction: Her knowledge helps her to do fundal pressure and controlled cord traction in correct direction according to the shape of the birth canal. Doing fundal pressure in a backward and downward direction. Controlled cord traction (CCT) when the placenta is high in downwards direction and as it descends in outward direction and when visible in an upward direction. This makes the delivery of the placenta easier with less risk of trapping and retained placenta or retained products of conception.
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowWe are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved