Obstetric Anatomy and Physiology
The Fetal Sac (Amnion and Chorion)
Table of Contents
THE FETAL SAC (AMNION AND CHORION)
The fetal sac consists of double membranes. The outer membrane is the chorion, and the inner membrane is the amnion, which contains the amniotic fluid as long as it remains intact. The intact membranes protect the fetus from ascending bacterial infection.
Chorion Membrane
The chorion membrane represents the remnant of the chorion laeve and ends at the margin of the placenta.
It is thicker than the amnion, friable, and shaggy on both sides.
Internally, it is attached to the amnion by loose areolar tissue and remnants of primitive mesenchyme.
Externally, it is covered by vestiges of the trophoblastic layer and the decidual cells of the fused decidua capsularis and parietalis.
The human placenta is, therefore, a discoid, deciduate, labyrinthine, and hemochorial type.
Amnion Membrane
The amnion is the inner layer of the fetal membranes.
Its internal surface is smooth and shiny and is in contact with the liquor amnii (amniotic fluid).
The outer surface consists of a layer of connective tissue and is opposed to the similar tissue on the inner aspect of the chorion, from which it can be peeled off.
The amnion can also be peeled off from the fetal surface of the placenta except at the insertion of the umbilical cord.
Structure of Amnion: Fully formed amnion is $0.02-0.5\text{mm}$ in thickness. From within outwards, the layers are: (1) single layer of cuboidal epithelium, (2) basement membranes, (3) compact layer of reticular structure, (4) fibroblastic layer, and (5) spongy layer. The amnion has neither blood nor nerve supply nor any lymphatic system.
Functions of the Amnion
Contribute to the formation of liquor amnii (amniotic fluid).
Intact membranes prevent ascending uterine infection.
Facilitate dilatation of the cervix during labor.
Has enzymatic activities for steroid hormonal metabolism.
Is a rich source of glycerophospholipids containing arachidonic acid (precursor of prostaglandin $\text{E}_2$ and $\text{F}_{2\alpha}$).
FUNCTIONS OF THE PLACENTA
1. Respiration
Since the respiratory system of the fetus is inactive, the interchange of gases takes place in the placenta by obtaining oxygen and getting rid of $\text{CO}_2$ through diffusion and osmosis (from low to high concentration).
2. Nutrition
Broken down food substances of important value are transported to the fetus through the placenta as end products, such as amino acids, fatty acids, and glucose. Other nutrients, such as calcium, phosphate, and vitamins, are obtained from the placenta to aid the growth of the fetus and the formation of red blood cells.
3. Storage
The placenta stores and metabolizes glucose in the form of glycogen and reconstitutes it to glucose as required. It also stores iron and fat-soluble vitamins.
4. Excretion
Waste materials from the fetus are carried through the semi-permeable membrane of the placenta to the mother’s blood circulation.
5. Endocrine Function
The chorionic villi, embedded in the decidua, secrete hormones which aid in the maintenance of pregnancy and growth of the fetus:
H.C.G. (Human Chorionic Gonadotropic Hormone): Produced by the cytotrophoblast layer at $7-10$ weeks and reduces as pregnancy advances. Its function is to stimulate the activity of the corpus luteum.
Oestrogen: Secreted throughout pregnancy.
Progesterone: Secreted from the syncytium until the onset of labor when its level falls.
6. Human Placental Lactogen (HPL)
HPL maintains glucose metabolism in pregnancy. It has a connection with the Human Growth Hormone, as its level rises and continues throughout pregnancy.
7. Stabilization
The chorionic villi, which are anchored by the decidua, hold the placenta firmly, stabilizing it. This stability is necessary for fetal growth.
8. Protection
The placenta provides a limited barrier to infection.
Exceptions include Treponema pallidum (syphilis) and TB (tuberculosis), as a few bacteria can penetrate.
Viruses, such as the rubella virus, can cross the placental barrier and cause congenital abnormalities.
Some drugs are known to cause damage, such as certain antibiotics given to the mother.
Immune globulin (IgG) is transferred to the fetus, providing the baby with passive immunity for the first three months after birth.
Note: Drugs like Fansidar affect the placenta and can cause jaundice in the baby, so they should not be given in the early weeks of gestation.
DEVELOPMENTAL ABNORMALITIES
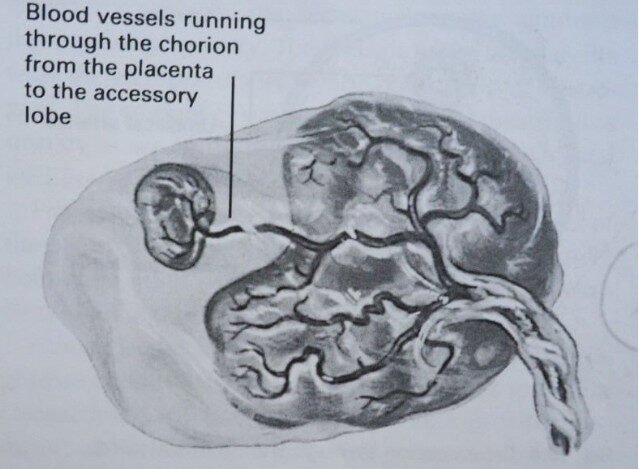
Succenturiate Lobe (Placenta Succenturiata)
This is the most significant abnormality and consists of an accessory lobe of placental tissue situated away from the main placenta. The accessory lobe is connected to the main placenta on the fetal surface by blood vessels traveling through the main placenta..
Dangers Associated with Succenturiata:
The lobe may be retained when the placenta is expelled, which may result in Postpartum Hemorrhage (P.P.H.) and interfere with uterine contractions during the third stage of labor.
The retained lobe may become infected, leading to puerperal sepsis and possibly secondary P.P.H.
There is a risk of Intra-uterine Fetal Anoxia as the fetus may compress the blood vessels connecting the lobe.
Sometimes the membranes may rupture and involve the connecting blood vessels, which can lead to fetal blood loss
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowWe are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved