Reproductive Health
Antenatal Care
Table of Contents
Definition
Antenatal care is a planned methodological care and supervision given to a pregnant woman by a midwife or obstetrician from the time the mother starts attending antenatal clinic until beginning of labour.
Systematic supervision (examination and advice) of a woman during pregnancy is called antenatal(prenatal) care.
Objective of ANC
To ensure a normal pregnancy resulting in the delivery of a healthy baby by a healthy mother.
Aims of Antenatal Care
● To monitor the progress of pregnancy in order to support maternal health and normal fetal development.
● To prepare the mother for labour, lactation and subsequent care for her baby.
● To detect early and treat appropriately high risk conditions be it medical or obstetrical that would endanger the life of the mother and the baby.
● To screen high-risk cases.
● To prevent, detect, and treat complications early.
● To continuously assess risk and provide ongoing primary preventive healthcare.
● To educate the mother about the physiology of pregnancy and labor using demonstrations, charts, and diagrams (mothercraft classes) to reduce fear and improve psychological well-being.
● To discuss with the couple the planned place, time, and method of delivery, and the care of the newborn.
● To counsel the couple on family planning and provide appropriate advice to those seeking medical termination of pregnancy.
This is Achieved By
● Developing a partnership with the woman.
● Providing a holistic approach to the woman’s care that meets her individual needs.
● Promoting awareness of the public health issues for the woman and her family.
● Exchanging information with the woman and her family enabling them to make informed choices.
● Being an advocate for the woman and her family, supporting her right to choose care that is appropriate for her own needs and those of the family.
● Recognize complications of pregnancy and appropriately referring to women within the multi- disciplinary team.
● Facilitating the woman to make an informed choice about methods of infant feeding and giving appropriate and sensitive advice to support her decision.
● Facilitating the woman and her family in their preparations to meet the demands of birth and making a birth plan.
● Offering health education for parenthood.
Activities Done in ANC
● Registration
● Booking (history taking)
● Special tests and investigations
● Health education
● Immunization
● Treatment of minor disorders
● Provision of supplements
● Examination i.e. physical and abdominal
● Orientation of mothers
● Formulating a birth plan
● Counseling.
● Referral of cases
Initial Assessment (Booking Day)
Objectives for Initial Assessment (Booking Visit)
To assess the level of health by taking a detailed history and offering appropriate screening tests.
To establish baseline data (blood pressure, urinalysis, uterine growth, and fetal development) for comparison as the pregnancy progresses.
To identify risk factors by accurately documenting past and present obstetric, medical, family, and personal history.
To provide an opportunity to discuss any concerns the woman may have.
To advise on maintaining the health of the mother and developing fetus throughout pregnancy.
To build a trusting, collaborative relationship between the woman and midwife.
To make appropriate referrals when additional healthcare or support needs are identified.
History Taking
I. Demographic Data
Name
Age
Address
Occupation
Next of Kin (NOK): Relationship, occupation, contact information.
Level of Education (LOE)
Tribe
Religion
Nearest health facility and distance from home.
II. Social History
Habits:
○ Smoking: (Include information on the risks of nicotine constricting blood vessels, leading to placental insufficiency, fetal hypoxia, small for gestational age (SGA) infants, and abortions. Advise on gradual reduction to avoid withdrawal symptoms.)
○ Alcohol: (Include information on the risks of trauma resulting in abortion, placental abruption, loss of appetite, malnutrition, and SGA infants.)
○ Marital Status: (Include inquiry about marital happiness and duration.)
Home Environment:
○ Housing (rented or owned), number of rooms and occupants.
○ Environmental hygiene.
○ Water and food sources.
III. Family History
Health status of woman’s parents and siblings (including cause of death if applicable).
Familial diseases (e.g., cancer, diabetes, cardiac disease, allergies).
Other serious illnesses (e.g., mental illness, pregnancy complications).
History of multiple pregnancies.
IV. Past Surgical History
Accidents involving the spine, pelvis, and lower limbs (potential impact on pelvic diameters).
Major operations (e.g., Cesarean section (C/S), pelvic operations).
Blood transfusions (risk of HIV/AIDS and isoimmunization).
V. Past Medical History
Medical conditions that may complicate pregnancy, labor, or the puerperium (e.g., sickle cell disease, diabetes mellitus (DM), hypertension (HTN)).
Childhood illnesses (e.g., rickets, poliomyelitis—potential impact on pelvic diameters).
Infectious diseases (e.g., tuberculosis (TB), Hepatitis B).
Sexually transmitted infections (STIs) (e.g., syphilis, gonorrhea).
VI. Gynecological History
Gynecological conditions (e.g., abortions, ectopic pregnancy, fibroids).
Gynecological operations (e.g., myomectomy, dilation and curettage (D&C), evacuation).
VII. Menstrual History
Menarche.
Cycle length.
Cycle interval.
Menstrual flow amount.
Dysfunctional uterine bleeding (DUB).
Premenstrual spotting.
VIII. Family Planning History
Methods used.
Complaints (if any).
Reasons for discontinuation (if applicable).
IX. Past Obstetrical History
Previous pregnancies (including abortions, stillbirths, and living children—note health and immunization status).
Interpregnancy intervals.
Gestational lengths.
Birth weights.
Fetal outcomes.
Labor lengths.
Presentations.
Delivery types.
Prenatal and postnatal complications.
Breastfeeding duration (if applicable).
Labor interventions (e.g., operative delivery, induction, assisted delivery, postpartum hemorrhage (PPH)).
Puerperium (normal or complications such as sepsis, PPH).
X. Present Obstetrical History
Gravidity.
Parity.
Living, Miscarried, Number of Pregnancies (LMNP).
Estimated Date of Delivery (EDD) (Include Naegele’s rule explanation and assumptions, including caveats about irregular cycles, conception timing, and breakthrough bleeding.)
Weeks of Amenorrhea (WOA)
XI. Present Health
Appetite (relationship to malnutrition and anemia).
Sleep (identify causes of sleep disturbances).
Micturition (note frequency, pain—consider urinary tract infections (UTIs)).
Bowel action (address constipation).
Note
Conclude the history by asking if the mother has anything else to share.
Investigations
On the first day, every woman should receive the following investigations;
● Blood Pressure
● Weight
● Height
● Urinalysis: Albumen (pre-eclampsia indicator), acetone (dehydration indicator), glucose (diabetes indicator).
● Rapid Plasma Reagin/Venereal Disease Research Laboratory (RPR/VDRL): Syphilis screening.
● HIV Screening: Prevention of Mother-to-Child Transmission (PMTCT).
● Blood Grouping
● Haemoglobin (Hb) Level: Assess for anemia (perform at booking, 32-34 weeks, and 36 weeks).
● Coombs Test: Detect blood antibodies.
Clinical Tests (Ongoing ANC Visits)
● Weight: Monitored at each visit. Expected weight gain: 12.5 kg total (4 kg in first 20 weeks, 8.5 kg in last 20 weeks). Excessive gain may indicate multiples, large fetus, polyhydramnios; insufficient gain suggests poor fetal growth.
● Height: Measured at booking or during labor if no prior ANC attendance. Normal range: 152-170 cm (below 150 cm suggests small pelvis; above 170 cm suggests narrow pelvis).
● Shoe Size: Below size 5 may indicate small pelvis; normal range: 5-8.
● Blood Pressure: Monitored at each visit. Normal range during pregnancy: 90/60 to 140/90 mmHg. A significant increase (≥30 mmHg systolic or ≥15-20 mmHg diastolic) warrants urine protein testing and assessment of symptoms (e.g., visual disturbances). The mother is asked how she feels generally, especially her sight (blurred vision), then referred to the doctor.
Physical Examination
This includes a review of the physical systems to ascertain the woman’s general health. The breasts, pelvis and abdomen receive particular attention. The examination is carried out systematically beginning with the head and ending with the pelvis and abdomen.
● General Appearance: Body type, weight, energy level, grooming, posture. Observed upon entry/seating.
● Head: Scalp condition, hair (treatment, pattern).
● Eyes: Conjunctiva (anemia), sclera (jaundice), vision, discharge.
● Nose: Sense of smell, bleeding, obstruction, growths, discharge.
● Oral Cavity: Toothache, dentures, lip condition, chewing/swallowing difficulties, tongue/gums (anemia), sense of taste.
● Ears: Discharge, hearing loss.
● Neck: Range of motion, palpate for swelling (salivary glands: parotid, submandibular, sublingual; thyroid; lymph nodes: superficial cervical, deep cervical, subclavicular). Observe jugular veins, thyroid pulsation. (Note: Thyroid enlargement may be due to iodine deficiency or normal pregnancy changes; distended jugular veins may indicate cardiac issues or anemia.)
● Upper Limbs: Size, length, skin texture, muscle wasting, palm color, nail capillary refill, edema.
● Chest: Respiratory effort (assess for respiratory problems).
● Breasts:
○ Inspection: Size, symmetry, shape, retraction, skin changes (redness, discoloration), nipple characteristics (prominence, dimpling, retraction), scars, cracks, sores, axillary extension.
○ Palpation: Detect masses or abnormalities. (Promotes breastfeeding and identifies abnormalities.)
● Back: Fungal infections, scars, sacral edema (potential pre-eclampsia/eclampsia indicator).
● Lower Limbs: Size, muscle wasting, joint pain/stiffness, calf pain, edema, varicose veins, extra digits, infections, tibial/ankle edema.
● Feet: Hygiene, fungal infections, nail condition (venous return, color), sole condition. Perform Homan’s sign (assess for deep vein thrombosis). Assess maternal effort.
● Vulva: Sores, warts, varicose veins, abnormal discharge. Observe for discharge upon coughing.
Abdominal Examination
It is carried out from 24 weeks gestation to establish and affirm that fetal growth is consistent with gestational age during pregnancy.
Aims
● Observe signs of pregnancy
● Assess fetal size and growth
● Assess fetal health (auscultation of fetal heart)
● Detect deviations from normal
● Diagnose fetal lie and presentation
● Locate fetal parts
Preparation/Procedure
● Ensure mother has emptied bladder (within 30 minutes)
● Ensure privacy
● Mother on couch
● Wash hands; expose only abdomen for palpation
Steps
● Inspection: Stand at foot of bed; while mother is on her back with abdomen exposed from the xymphy sternum up to the symphysis pubis. Look at the size, shape, operational scars, signs of pregnancy like darkening of linea nigra below and above the umbilicus, fetal movements, Striae gravidurum etc.
● Palpation (Leopold’s Maneuvers): Stand at right side; use pads of fingers:
○ Superficial palpation (localized tenderness)
○ Hypochondriac palpation (enlarged organs)
○ Fundal height estimation
○ Pelvic palpation (presentation)
○ Fundal palpation (lie)
○ Lateral palpation (position)
NOTE: During a deep pelvic palpation, a midwife grips the fetal head between the thumb and fingers to check for engagement, this maneuver is termed as pawlik’s grip/second pelvic grip.
● Auscultation: This is the way of listening the fetal heart to determine fetal wellbeing by use of feto- stethoscope.
Abdominal Summary
● Fundal height
● Presentation
● Lie
● Position
● Fetal heart rate
Case Summary
● Comment on history, general and abdominal examination.
● Feedback
● Advice
● Return date
Ongoing Antenatal Care (ANC)
Purpose
● To continue to observe maternal health and freedom from infections.
● To assess fetal wellbeing.
● To ascertain that fetus has adopted a lie and presentation that will allow vaginal delivery.
● To offer an opportunity to express any fear or worries about pregnancy and labour.
● To ensure that mother and family are confident to decide when labour starts.
● To discuss any views about the conduct of labour and formulate a birth plan if required.
Risk Factors During Pregnancy
● Change in fetal movement pattern
● Hb < 10g/dl
● Poor weight gain/loss
● Proteinuria
● BP > 140/90 mmHg
● Uterus size discrepant with dates
● Excess/decreased amniotic fluid
● Malpresentation
● Vaginal bleeding
● Premature contractions
● Vaginal infection
● Head not engaged by 38 weeks
For PG; On Each Visit: do the following
● Review card; assess past complaints.
● Take BP, weight; test urine.
● Carry out general and abdominal examinations.
● Administer medications as needed.
Indicators of Fetal Wellbeing
● Increased maternal weight with increasing uterine size.
● Regular fetal movement pattern.
● Fetal heart rate 120-160 bpm.
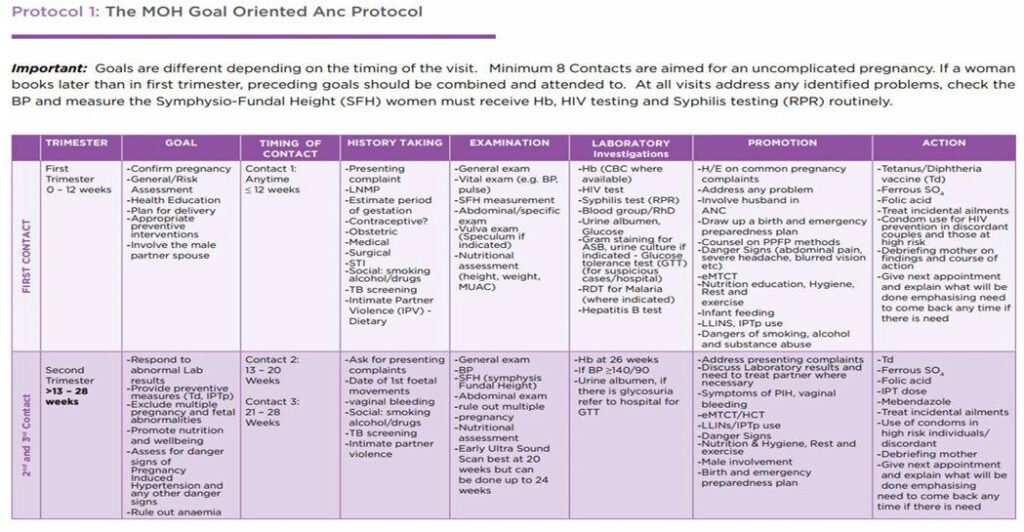
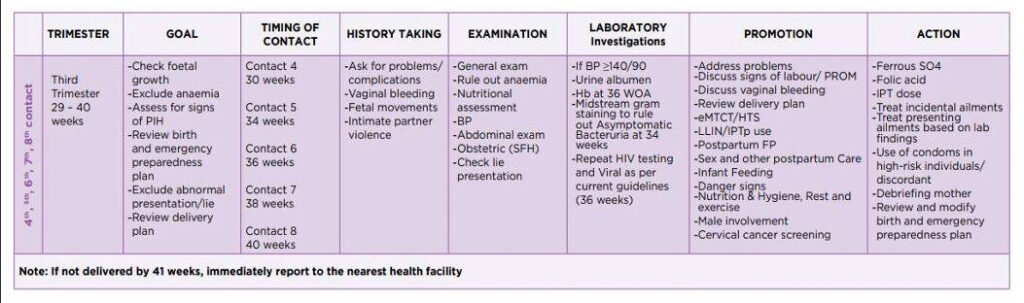
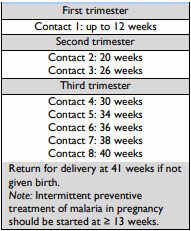
Goal Oriented Antenatal Care
Goal oriented ANC is an approach to ANC that is evidence-based, goal-directed, individualized, woman-centred care and emphasises quality versus quantity of visits and care by skilled providers.
It ensures provision of adequate care to a pregnant woman from the time pregnancy is diagnosed up to the time of delivery. During this time the pregnant woman is prepared for a safe delivery of a mature normal baby.
Pelvic Capacity (from Labor Context, Related to ANC)
● While ideally assessed during antenatal care (ANC), the midwife should reassess pelvic adequacy during the vaginal examination.
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowWe are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved