Medical Nursing (III)
Subtopic:
Gout
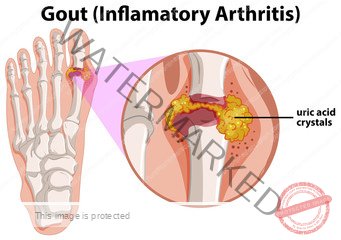
Gout is a metabolic disorder distinguished by elevated levels of uric acid in the blood and the formation of urate crystal deposits within the fluid of joints and surrounding tissues.
The origin of the term “Gout” is from the Latin word “Gutta,” which translates to a “drop” (of liquid).
Gout is also a type of arthritis that occurs when uric acid accumulates in the bloodstream, leading to inflammation in the joints. This condition can be either acute or chronic.
Acute: The affected joints often appear red and swollen and are tender to the touch. The pain is often described as a burning sensation. The start of acute gout is commonly triggered by factors such as injury, alcohol consumption, surgical procedures, and systemic infections.
Chronic: This stage is marked by visible deposits of urate crystals (tophi), which form nodules that can be painful during gout attacks.
Cause
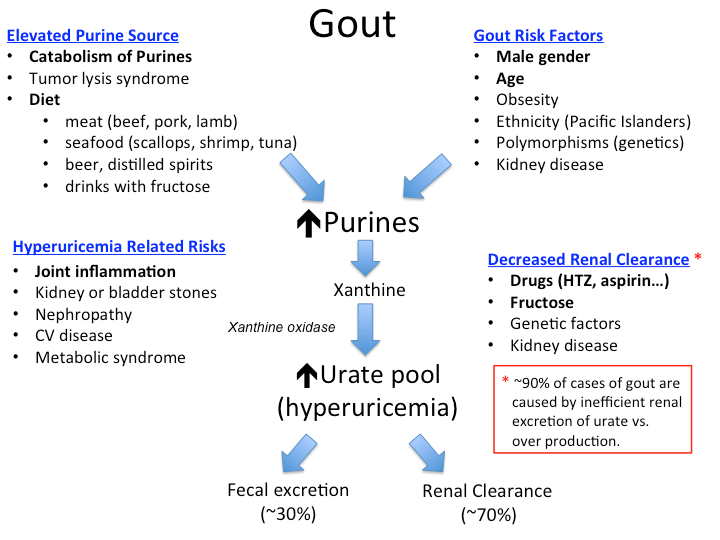
Gout is connected to the presence of hyperuricemia (meaning high levels of urate in the blood, or when serum urate levels are greater than about 6.8 mg/dL).
Hyperuricemia: Gout develops when urate crystals accumulate within a joint, causing the inflammation and intense pain associated with a gout attack. Urate crystals can form when there are high amounts of uric acid present in the bloodstream.
NOTE: It’s important to know that not everyone with hyperuricemia will develop gout. The condition requires two key processes to occur – crystallization and inflammation. When uric acid levels become too high, crystals will form in the joints, which then initiates the inflammatory process.
Risk Factors
Gender: Gout is more frequently seen in males compared to females. Men typically have higher urate levels than women.
Obesity: Having excess body weight increases the risk of gout.
Age: As age increases, there’s often a decrease in kidney function and an increased use of diuretic medications, both of which can interfere with the body’s ability to remove urate.
Having certain health conditions, including:
Congestive heart failure
Hypertension (high blood pressure)
Insulin resistance
Metabolic syndrome
Diabetes
Poor kidney function
Using certain medications, such as thiazides and loop diuretics, as they can interfere with the way the kidneys clear urate by affecting various transporters in the proximal renal tubule. Even aspirin can inhibit urate secretion and increase serum urate levels at commonly used dosages.
Drinking alcohol: The risk of gout increases as alcohol intake increases.
Eating or drinking food and drinks high in fructose (a type of sugar). Blood uric acid levels can rise quickly after consuming fructose.
Having a diet high in purines, which the body breaks down into uric acid. Examples of purine-rich foods include red meat.
Family history of Gout: Having relatives with gout increases your risk.
Chemotherapy-induced tumor lysis syndrome: This occurs when the rapid breakdown of cancer cells during chemotherapy leads to a large increase in urate.
Signs & Symptoms of Gout
Podagra: This refers to sudden episodes of arthritis affecting the big toe. The big toe is the most common site for painful gout-related inflammation due to a combination of factors: a slightly lower temperature, lower pH, and a certain level of dehydration.
temperature: The joint at the base of the big toe has a slightly lower temperature, which makes it easier for crystals to form.
pH: Physical injury can cause a more acidic environment (lower pH), which also promotes crystal formation.
level of joint hydration: Dehydration within the joint, especially at night, can cause crystals to form, which may explain why gout pain often starts during the night.
Tophi (the plural form of tophus): These are collections of urate crystals that form in individuals who have had high uric acid levels for a long time. They are most often found in joints, cartilage, and bones.
Urate kidney stones forming in the ureter (urolithiasis). These are more likely to occur in individuals with acidic urine.
Nephropathy: Kidney damage can occur due to urate crystal deposits in the renal medulla in severe cases of gout.
Other signs and symptoms include:
The start of pain is often at night, with sudden swelling and intense pain.
Joint pain usually builds over two to four hours and often occurs during the night.
A low-grade fever may be present.
Symptoms typically get better within 2 to 10 days.
Stages/ Phases of Gout
The progression of gout can be described in four phases: asymptomatic hyperuricemia, acute gouty arthritis, intercritical gout, and chronic tophaceous gout.
ASYMPTOMATIC HYPERURICEMIA
Asymptomatic hyperuricemia refers to the condition of having an abnormally high level of urate in the blood, but without experiencing gouty arthritis or kidney stones. In this initial stage of gout, the person does not have joint pain, or red or swollen joints, only an elevated uric acid level shown in a blood test.
ACUTE GOUTY ARTHRITIS
Acute gout is marked by the sudden onset of pain, redness, limited movement, and swelling in the affected joint. This happens when urate crystals are released into the joint fluid, causing an inflammatory reaction, which involves many white blood cells and the release of inflammatory chemicals that cause the pain, redness, and swelling.
INTERCRITICAL GOUT
After recovering from acute gouty arthritis, the patient enters a period without symptoms. This phase is known as “intercritical gout.” During this phase, the person has had a gout attack in the past but is currently not experiencing any joint pain or swelling, and has no other signs or symptoms of gout.
RECURRENT GOUTY ARTHRITIS (Chronic or Tophaceous Gout)
In this stage, uric acid deposits can form nodules called “tophi,” often found at the bunion area of the big toe or at the elbow. This stage is characterized by persistent joint pain from gout, nearly all the time. It typically takes many years of poorly controlled gout for someone to reach this stage.
During this stage, progressive damage to the joints develops, so it’s important for patients with gout to receive treatment before this occurs.
The likelihood of having more acute gout attacks usually increases over time. Approximately 60 percent of patients will have a second attack within the first year, and 78 percent will have a second attack within two years. Only 7 percent of patients will not have another attack within a 10-year period.
Pathophysiology of Gout
Normal, healthy joints possess a lining called the synovial membrane, which contains specialized cells resembling fibroblasts and macrophages. These cells are crucial for maintaining the joint’s internal balance, including supplying nutrients and producing a clear, viscous fluid. This fluid acts as a lubricant, minimizing friction between the cartilage surfaces during movement.
During periods of hyperuricemia, when urate crystals form within the joint, they become coated with proteins. This protein coating significantly amplifies their pro-inflammatory properties. Furthermore, it is thought that this protein layer may impede the urate crystals from being cleared from the joint area.
The presence of these protein-coated urate crystals triggers a cascade of events. This includes the engulfment (phagocytosis) of the urate crystals by cells, the activation of signaling pathways on the surface of cells within the synovial membrane, and the subsequent release of various inflammatory messengers called cytokines.
Crucially, cytokines released by cells within the joint, particularly interleukin-1 beta (IL-1β), initiate chemotaxis. This is the process of attracting and activating neutrophils, monocytes, and numerous other types of inflammatory cells to the affected area. Once these neutrophils and other inflammatory cells are inside the joint, they interact directly with the urate crystals. This interaction prompts the release of additional inflammatory mediators such as prostaglandins, nitric oxide, leukotrienes, and other substances. These mediators contribute to both the direct damage of tissues within the joint and the increased sensitivity of pain receptors, resulting in intense pain.
Diagnostic Tests / Investigations
Joint fluid test: A procedure involving the extraction of fluid from the affected joint using a needle. Examination of this fluid under a microscope can reveal the presence of urate crystals, offering a highly reliable confirmation of a gout diagnosis.
Blood test: Gout arises from an excess of uric acid, a natural waste product, in the bloodstream, leading to crystal formation in the joints. A blood test indicating elevated uric acid levels can support a gout diagnosis, although it is not definitively diagnostic on its own.
X-ray imaging: X-rays of the affected joint are valuable for excluding other potential causes of joint inflammation.
Ultrasound: This imaging technique utilizes sound waves to identify urate crystals within the joints and detect tophi – deposits of uric acid crystals that manifest as hard, visible lumps in or near the joints.
Dual-energy computerized tomography (DECT): This advanced imaging technique combines X-ray images taken from multiple angles, providing a detailed visualization of urate crystals within the joints.
Creatinine: This blood or urine test measures the levels of creatinine, a waste product produced by muscle activity. Abnormal levels can be an indicator of underlying kidney disease.
Blood Urea Nitrogen (BUN): Often performed alongside the creatinine test, the BUN test assesses the blood levels of urea nitrogen, another waste product typically eliminated by the kidneys. Elevated levels may suggest that the kidneys are not functioning optimally.
Urinalysis: A urine test may be conducted to check for high levels of uric acid, which could indicate an increased risk of developing kidney stones.
Management of Gout
Aims:
To effectively relieve the pain and inflammation associated with acute gout attacks.
To lower the overall levels of uric acid in the body.
To prevent the development of long-term complications.
Medical Management:
The primary focus of acute gout treatment is to address the intense pain and inflammation caused by the accumulation of urate crystals in the joints, most commonly affecting the big toe.
It’s crucial to understand that while anti-inflammatory medications effectively manage the symptoms of acute attacks, they do not lower uric acid levels and therefore do not prevent ongoing joint damage or the formation of kidney stones. Consequently, anti-inflammatory agents are not suitable for long-term therapy in patients who are appropriate candidates for urate-lowering treatment.
There are three main categories of anti-inflammatory medications used for the acute treatment of gout:
NSAIDs
COLCHICINE
GLUCOCORTICOIDS (Corticosteroids)
NSAIDs e.g.
Naproxen, Ibuprofen (available without a prescription)
Indomethacin (a more potent NSAID requiring a prescription)
Indication: To treat inflammation and pain associated with acute gout attacks.
Mechanism of Action: NSAIDs work by non-selectively inhibiting cyclooxygenase (COX) enzymes, specifically COX-1 and COX-2. This inhibition reduces the production of prostaglandins, which are key mediators of inflammatory responses and pain in gout.
Relative contraindications:
Renal insufficiency (inhibiting prostaglandin synthesis can potentially lead to kidney failure).
Peptic ulcer (increased risk of gastrointestinal bleeding).
Cardiovascular (CV) disease (increased risk of stroke or myocardial infarction).
Known allergy to NSAIDs.
Concurrent use of other anticoagulant medications (increased risk of bleeding).
COLCHICINE:
Used to reduce pain and inflammation during acute gout attacks. It is most effective when taken at the very first sign of joint discomfort, targeting the early stages of neutrophil recruitment and activation.
Colchicine treatment is generally reserved for patients who have contraindications to NSAIDs or who do not respond adequately to NSAIDs.
It can be used in combination with NSAIDs in certain cases.
GLUCOCORTICOIDS (Corticosteroids):
Offer an alternative for patients who have contraindications to both NSAIDs and colchicine.
Can be administered directly into the affected joint (intra-articular injection), orally, or parenterally (injection outside the digestive tract), with the chosen route depending on the severity of symptoms and the number of affected joints.
Combination Therapy:
Combination therapy may be considered for patients experiencing severe pain or pain that is not sufficiently relieved by a single medication. Common combinations include:
Colchicine + NSAID
Colchicine + oral glucocorticoid
NSAID + intraarticular glucocorticoid
Colchicine + intraarticular glucocorticoid
Oral glucocorticoid + intraarticular glucocorticoid
Lowering uric acid in the body:
XANTHINE OXIDASE INHIBITORS:
* These are typically the first-line drug therapy recommended for long-term management. They work by reducing the production of uric acid from purines.
* Allopurinol (Zyloprim ®) is a commonly used xanthine oxidase inhibitor and is a purine analog.
* It is important to note that allopurinol is “not an innocuous drug” and is recommended for symptomatic hyperuricemia only.
* Administering colchicine or NSAIDs concurrently during the initial 3-6 months of urate-lowering therapy has been shown to decrease the likelihood of flare-ups.
* N.B. Allopurinol carries a risk of rare but serious, potentially life-threatening drug hypersensitivity reactions (e.g., Stevens-Johnson syndrome and DRESS syndrome). Allopurinol is one of the most frequent causes of these severe reactions.
URICOSURICS:
* Uricosuric drugs are organic acids that function by inhibiting the reabsorption of uric acid in the kidneys. They achieve this by blocking anionic transport sites in the renal proximal tubule. By preventing reabsorption, these drugs enhance the clearance of uric acid from the body. Probenecid is the primary uricosuric drug available.
* Probenecid is used for patients who cannot tolerate allopurinol or require additional urate lowering. It can be used in combination with a xanthine oxidase inhibitor.
* It is often administered alongside colchicine to reduce the risk of gouty flare-ups.
* Probenecid can lower average serum uric acid levels by 30-40%.
* It is not effective in patients with significant kidney dysfunction.
* Probenecid can increase the risk of kidney stone formation in individuals with high levels of uric acid in their urine and is contraindicated in patients with a history of kidney stones (nephrolithiasis).
URICOSLYTICS:
* These medications work by converting uric acid into a more water-soluble metabolite, facilitating its removal from the body.
* Pegloticase (Krystexxa ®) is typically reserved for the treatment of severe, chronic gout that has not responded to other therapies.
* While Pegloticase effectively lowers uric acid levels, its ability to reduce the frequency of recurrent gout attacks and the optimal duration of therapy are not fully understood.
* Uricase (or uric acid oxidase) is an enzyme present in most organisms, but the gene for this enzyme is non-functional in humans. It converts uric acid into allantoin, a metabolite that is 5-10 times more water-soluble than uric acid.
* Pegloticase infusions, typically given every 2 weeks, are effective in lowering uric acid levels. However, its use is limited by cost, the potential for infusion reactions, and the development of tolerance, which may be due to the formation of antibodies against the drug.
Surgical Management:
In cases where gout symptoms have persisted without adequate treatment, uric acid crystals can accumulate in the joints, forming gritty, chalky nodules known as tophi.
These tophi can lead to infection, pain, pressure, and joint deformities. Surgical excision to remove the tophi may be recommended in these situations.
Patient advice:
Reduce fructose consumption:
Limit sweetened soft drinks and fruit juices.
Avoid foods containing high fructose corn syrup, such as ice cream, desserts, and syrup.
Avoid high purine foods:
Avoid consuming organ meats (kidney, liver, sweetbreads).
Limit serving sizes of beef and pork.
Reduce alcohol intake:
Reduce consumption of wine and spirits, and avoid all alcohol intake during gout attacks.
Beer contains purines, and alcohol consumption can lead to the production of lactic acid, which interferes with urate clearance.
Weight loss for obese patients:
Modify diet and increase exercise to achieve a healthy BMI.
Weight loss can improve the kidneys’ ability to excrete urate.
Encourage consumption of:
Low-fat or non-fat dairy products.
Vegetables.
Eliminating unnecessary drugs:
Many medications, including thiazides, loop diuretics, niacin, and aspirin, can contribute to hyperuricemia. In some cases, suitable alternatives or dosage reductions may be possible, but the therapeutic benefits must be carefully considered.
Nursing Management using Nursing Process:
Assessment: Acute Pain:
Sudden and severe pain in one or more joints, typically the big toe, is the hallmark symptom of gout. This excruciating pain arises from the accumulation of uric acid, forming sharp crystals within the joint.
Nursing Diagnosis: Acute Pain related to the Inflammatory process as evidenced by:
Reddened, swollen joints, Distraction behavior, Expressive behavior, Guarding behavior, Positioning to ease pain, Limited range of motion, Reports pain characteristics and intensity.
Expected Outcome:
The patient will verbalize pain relief and perform activities of daily living without discomfort.
The patient will display an absence of redness, swelling, and warmth to the affected joints.
Interventions:
Administer pain medications as indicated:
NSAIDs are commonly prescribed to alleviate pain and reduce joint inflammation in gout patients. Steroids can also be beneficial in reducing joint damage.Elevate the limb:
Elevating the affected joint can help minimize inflammation.Apply cool compresses:
Non-pharmacological interventions, such as applying cool compresses or ice packs, can help reduce inflammation and soothe burning sensations.Adjust lifestyle behaviors:
Gout attacks can be minimized by addressing modifiable risk factors, such as reducing the intake of alcoholic beverages, sugary drinks, and high-purine foods like red meats and certain seafood.
Assessment: Impaired Physical Mobility:
Patients with gout often experience difficulty walking or standing, particularly during flare-ups affecting the feet, knees, or ankles, due to severe and sudden pain and swelling. Joint swelling can lead to stiffness and pain upon movement, resulting in a limited range of motion.
Nursing Diagnosis: Impaired Physical Mobility related to: Pain, Inflammatory process, Limited range of motion, Joint tenderness, Joint stiffness as evidenced by:
Altered gait, Decreased range of motion, Difficulty turning, Slowed movement, Spastic movement, Uncoordinated movement, Hesitancy to move.
Expected outcomes:
The patient will be able to ambulate with minimal discomfort.
The patient will participate in activities to improve their range of motion.
Interventions:
Encourage weight loss:
Obesity places additional stress on joints and increases the risk of developing diabetes, hypertension, and other chronic conditions that are also risk factors for gout.Encourage active and passive ROM exercises:
Range of motion exercises help maintain the flexibility and mobility of the affected joints. Gout can cause joint stiffness, and providing patients with exercises they can perform independently or with assistance can help maintain their mobility.Refer to PT or OT:
A physical therapist (PT) or occupational therapist (OT) can conduct a thorough evaluation of the extent of impaired physical mobility in gout patients and develop tailored interventions.Encourage the use of mobility aids when necessary:
Mobility aids, such as handrails, canes, and shower benches, enhance patient safety during gout flare-ups and help prevent accidental falls and other injuries.
We are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved