Skin conditions
Subtopic:
Onychomycosis

Onychomycosis is the medical term for a fungal infection affecting the nails. This condition is quite prevalent, accounting for as much as 20% of all reported nail disorders.
While onychomycosis can affect both fingernails and toenails, infections of the toenails are particularly common due to the often warm and moist environment within shoes, which encourages fungal growth.
The most frequent cause of onychomycosis, responsible for approximately 80-90% of cases, is a group of fungi known as dermatophytes. This specific type of fungal nail infection caused by dermatophytes is also referred to as tinea unguium, which literally translates to “tinea of the nails.”
The presence of onychomycosis can lead to a number of visible changes in the affected nails, including:
Discoloration: The nail may change color, often becoming white, yellow, brown, or even black.
Thickening: The nail plate can become abnormally thick and overgrown.
Chalkiness: The nail may develop a powdery, chalk-like texture or appearance on its surface.
Crumbling: The nail can become brittle and prone to breaking or crumbling at the edges or throughout the nail plate.
Treatment for onychomycosis often involves the use of potent oral antifungal medications, as topical treatments may not effectively penetrate the nail to reach the infection.
Classification of Onychomycosis
Onychomycosis is categorized based on the observed pattern of nail bed involvement. The primary types include:
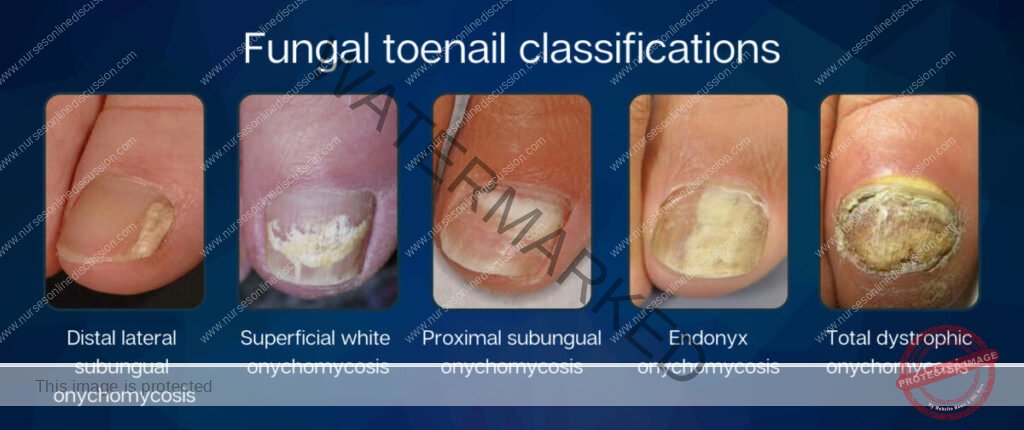
Distal and Lateral Subungual Onychomycosis (DLSO): This is the most frequently encountered form of tinea unguium, typically caused by Trichophyton rubrum. The fungus invades the nail bed and the underside of the nail plate, progressing from the distal (far end) and lateral (sides) aspects.
Superficial White Onychomycosis (SWO): This type occurs when fungi invade the upper layers of the nail plate, leading to the formation of characteristic “white islands” or patches on the nail surface. SWO accounts for approximately 10% of all onychomycosis cases.
Proximal Subungual Onychomycosis (PSO): In PSO, fungi penetrate the newly developing nail plate through the proximal nail fold (the skin at the base of the nail). This is the least common form of tinea unguium in healthy individuals but is observed more frequently in immunocompromised patients.
Endonyx Onychomycosis (EO): With EO, the fungus penetrates throughout the entire thickness of the nail plate directly from underneath the surface of the nail. Notably, the nail bed itself is not infected in this type. EO is more commonly seen in individuals with compromised immune systems.
Total Dystrophic Onychomycosis (TDO): This represents the most severe form of onychomycosis, characterized by complete destruction of the nail plate. TDO is the ultimate outcome of any of the other four types of onychomycosis if left untreated or if the infection progresses significantly.
Causes of Onychomycosis
The primary causative agents of onychomycosis are fungi known as dermatophytes.
Trichophyton rubrum is the single most common dermatophyte responsible for these infections.
Other dermatophytes, such as Trichophyton interdigitale and Epidermophyton floccosum, can also cause onychomycosis.
Dermatophytes are identified in the majority of onychomycosis cases, accounting for approximately 90% of toenail and 50% of fingernail infections.
Candida albicans, a type of yeast, is responsible for about 2% of onychomycosis cases, particularly affecting fingernails.
Yeasts are more commonly the cause of fingernail onychomycosis, particularly in individuals whose hands are frequently immersed in water.
Risk Factors
Several factors can increase the likelihood of developing onychomycosis:
Age: Aging is the most significant risk factor. This may be attributed to factors such as previous nail trauma, reduced nail care, and impaired peripheral circulation.
Family history: Having a family history of onychomycosis increases an individual’s susceptibility.
Warm and moist environments: Conditions that promote moisture around the nails, such as wearing tight-fitting shoes, create a favorable environment for fungal growth.
Walking barefoot in public areas: Exposure to fungi is higher in communal areas like swimming pools, public baths, and showers.
Pre-existing nail conditions: Conditions like tinea pedis (athlete’s foot), nail injury, nail damage, and psoriasis can predispose individuals to onychomycosis.
Conditions affecting peripheral circulation: Medical conditions associated with poor blood flow to the extremities, such as diabetes mellitus and peripheral arterial disease, increase risk.
Immunodeficiency: Conditions that weaken the immune system, such as cancer, post-transplant status, HIV infection, and undergoing chemotherapy or radiotherapy, make individuals more vulnerable to fungal infections.
Clinical Presentation
The hallmark of onychomycosis is the presence of distorted nails. Common clinical features include:
Changes in nail texture and discoloration.
Thickening of the nail plate, which may appear yellow or cloudy.
The nails can become rough and crumbly, or the nail plate may separate from the nail bed (onycholysis).
In some cases, the infected nail may have a slightly foul odor (malodor).
Complications
Although often considered a cosmetic issue, onychomycosis can lead to more serious complications, including:
Cellulitis (bacterial skin infection)
Sepsis (blood infection)
Osteomyelitis (bone infection)
Tissue damage surrounding the nail
Permanent loss of the affected nail
Management / Treatment of Onychomycosis
Treatment typically involves the use of oral antifungal medications. Effective options include:
Oral antifungal medications: Terbinafine, itraconazole, and fluconazole are commonly prescribed systemic antifungals.
Preferred treatment regimens:
Terbinafine: 250 mg orally once daily (OD) for adults. For children, the dosage is weight-based: <20 kg: 67.5 mg/day, 20–40 kg: 125 mg/day, >40 kg: 250 mg/day, for a duration of 6 weeks.
Itraconazole: 200 mg orally once daily (O.D) for 3 months.
Fluconazole: 150–300 mg orally once weekly for 6–12 months.
Fungal laser therapy: Laser treatments aim to inhibit fungal reproduction (fungistatic effect) or directly kill the fungus (fungicidal effect).
Prevention of Onychomycosis
Adopting preventive measures can significantly reduce the risk of developing onychomycosis:
Wear properly fitting shoes: Shoes that are either too tight or too loose can cause trauma to the toenails, creating entry points for fungal organisms.
Avoid being barefoot in public areas: Minimize exposure by wearing footwear in communal spaces frequented by barefoot individuals, such as public swimming pools, locker rooms, showers, and hotel rooms.
Proper nail care: Avoid picking or tearing at toenails. Use clean instruments to trim toenails straight across, avoiding rounded edges. Trauma from improper cutting can create entry points for fungi.
Thoroughly dry feet: Ensure feet, including the areas between the toes, are completely dry after showering or bathing.
Keep feet dry: Maintain dry feet throughout the day and avoid wearing damp shoes.
Avoid sharing barefoot spaces: If family members have foot or toenail fungal infections, avoid sharing common spaces without footwear.
Foot care for specific conditions: If you have diabetes or reduced blood flow to the feet, adhere to recommended foot care exercises and guidelines provided by your healthcare provider.
We are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved