Specialized Nursing Care Procedure
Subtopic:
Introduction to Ophthalmology

Learning Objectives
Define the roles of key ophthalmic professionals: ophthalmologist, optometrist, optician, and ophthalmic nurse.
Describe the responsibilities of ophthalmic nurses in routine care, surgical assistance, and patient education.
Identify and categorize ophthalmic emergencies and conditions requiring urgent or prompt attention.
Explain the principles and procedures involved in maintaining eye hygiene and preventing complications.
List conditions that necessitate eye care interventions, including infections, trauma, surgery, and systemic diseases.
Summarize the goals and applications of eye medications used for infection control, lubrication, and post-surgical care.
Ophthalmology
Ophthalmology is the branch of medicine that deals with the anatomy, physiology, and diseases of the eye. It encompasses the diagnosis, treatment, and prevention of eye diseases and disorders, as well as vision correction.
Definitions of Ophthalmic Professionals
Ophthalmologist: A medical doctor (MD) or doctor of osteopathic medicine (DO) specializing in the medical and surgical care of the eyes. They diagnose and treat all eye diseases, perform eye surgery, prescribe and fit eyeglasses and contact lenses, and may conduct research on eye diseases and vision disorders.
Optometrist: A healthcare professional who provides primary vision care, including sight testing, vision correction, and the diagnosis, treatment, and management of vision changes. They are not medical doctors but are Doctors of Optometry (OD).
Optician: A technician trained to design, verify, and fit eyeglass lenses and frames, contact lenses, and other vision-correcting devices.
Ophthalmic Nurse: A registered nurse with specialized training in ophthalmology, who assists in the assessment, treatment, and care of patients with eye conditions.
Role of Ophthalmic Nurses
Ophthalmic nurses play a vital role in providing comprehensive eye care. Their responsibilities include:
Emergency Care: Providing first aid for eye injuries and emergencies.
Initial Assessment: Performing preliminary physical examinations, including blood pressure checks, to identify underlying health conditions that may affect eye health.
Patient Screening: Conducting initial vision screenings.
Medical History: Collecting detailed patient medical histories.
Assisting with Examinations: Assisting ophthalmologists during eye examinations.
Patient Education: Providing guidance on managing eye pain, administering medications, and treating ocular conditions.
Surgical Preparation and Assistance: Preparing patients for eye surgery and assisting during the procedure.
Post-operative Care: Providing care and monitoring after eye surgery.
Performing Eye Tests: Conducting various eye tests and procedures, as directed by the ophthalmologist.
Ophthalmic Emergencies and Urgent Cases
Ophthalmic Emergencies and Conditions Requiring Prompt Care
Emergencies Demanding Immediate Medical Intervention:
Sudden Vision Loss:
Central Retinal Artery Occlusion: This occurs when the main artery delivering blood to the retina becomes obstructed, leading to a sudden and severe loss of vision.
Central Retinal Vein Occlusion: In this condition, the primary vein responsible for draining blood from the retina is blocked, resulting in visual impairment.
Giant Cell Arteritis: This inflammatory disorder affects the arteries, particularly those in the head, including the ones that nourish the eye. It can cause sudden vision loss.
Retinal Detachment: This happens when the retina, the light-sensitive tissue at the back of the eye, separates from its underlying layers, potentially resulting in significant vision loss, particularly if the macula (the central area of the retina responsible for sharp vision) remains attached.
Primary Acute Glaucoma: This condition is characterized by a sudden and significant elevation in intraocular pressure (pressure within the eye), which can lead to severe pain, blurred vision, and the perception of halos around lights.
Trauma:
Penetrating or Perforating Injuries: These involve objects piercing the eye, posing a serious risk of vision loss and infection.
Chemical Burns: Exposure to caustic chemicals can cause severe damage to the eye’s surface.
Orbital Cellulitis: This is a serious infection of the tissues surrounding the eye, which can spread rapidly and lead to vision loss and other complications.
Conditions Requiring Prompt, But Not Necessarily Immediate, Attention:
Corneal Ulcer: An open sore on the cornea (the clear, front part of the eye) can cause pain, redness, light sensitivity, and blurred vision.
Vitreous Hemorrhage: Bleeding into the vitreous humor (the gel-like substance that fills the back of the eye) can cause blurred vision and the appearance of floaters or “cobwebs” in the visual field.
Acute Dacryocystitis: This refers to inflammation of the lacrimal sac (the tear sac), which can lead to pain, swelling, redness, and tearing in the inner corner of the eye.
Optic Nerve Disorders: Various conditions affecting the optic nerve, which transmits visual information from the eye to the brain, can lead to visual disturbances, including vision loss.
Ocular Tumors: Growths within or around the eye can impact vision and may require treatment.
Acute Uveitis: Inflammation of the uvea (the middle layer of the eye, containing the iris, ciliary body, and choroid) can cause pain, redness, light sensitivity, and blurred vision.

Eye Care
Eye care involves specific practices to maintain eye health and prevent complications. This is particularly crucial for individuals whose natural eye cleansing mechanisms are compromised.
Natural Eye Cleansing and Its Importance
The eyes naturally cleanse themselves through tear production and blinking, as noted by Harrison in 2006. When this process is disrupted, intervention is needed to clear debris, ensure hydration, and maintain eyelid closure, as highlighted by Dawson in 2005.
Procedures Involved in Eye Care
Eye care may involve several procedures, including:
Cleansing: Gently cleaning the eye area.
Swabbing: Using sterile swabs to remove discharge or apply medication.
Medication Instillation: Administering eye drops or ointments.
Padding/Dressing/Shield Application: Protecting the eye with appropriate coverings.
Conditions Necessitating Eye Care
Various situations require diligent eye care, including:
Pre- and Post-Operative Eye Surgery: To maintain a clean, infection-free environment and prepare for surgical intervention.
Impaired Eyelid Closure: Conditions like hydrocephalus, cerebral palsy, facial nerve palsy, and other health conditions affect eyelid function and compromise natural eye protection.
Unconscious, Sedated, or Muscle-Relaxed Patients: These individuals lack the ability to blink or close their eyes, necessitating artificial lubrication and protection.
Eye Infections (e.g., Conjunctivitis): To control and eliminate infection, prevent its spread, and facilitate healing.
Non-Infected Sticky Eye (e.g., Blocked Tear Ducts): To clear discharge and reduce the risk of secondary infections.
Immunocompromised Patients: To prevent opportunistic infections in individuals with weakened immune systems.
Eye Trauma: To remove debris, manage pain, and prevent infection after injury.
Chronic Dry Eye: To provide lubrication and prevent corneal and conjunctival damage.
Post-Chemotherapy/Radiation Therapy: To address dryness and irritation caused by cancer treatments.
Congenital Eye Disorders (e.g., Ptosis, Congenital Glaucoma): To manage symptoms, prevent complications, and support eye health.
Post-Cataract Surgery: To ensure proper healing, prevent infection, and manage post-operative issues.
Severe Allergies: To alleviate irritation and discharge through regular cleaning and medication.
Exposure to Environmental Irritants: To remove irritants like smoke, dust, or chemicals.
Objectives of Eye Care
The primary goals of eye care are to:
Maintain Cleanliness: Promote patient comfort and reduce cross-infection risk.
Prevent Dryness: Utilize various methods like methylcellulose drops, ointments, general lubricants, polyacrylamide hydrogel dressings, and hypromellose drops (artificial tears) to maintain moisture.
Ensure Eyelid Closure: Employ polyacrylamide hydrogel dressings (e.g., Geliperm®) to keep eyelids closed in patients unable to do so naturally.
Treat Infections: Clean the eye and administer appropriate medications.
Enhance Medication Efficacy: Ensure the eye is clean before medication administration.
Protect Eyes During Phototherapy: Shield the retina from light exposure, particularly in newborns with jaundice.
Support Post-Surgical Healing: Reduce infection risk and manage discomfort after procedures like cataract removal.
Manage Allergic Reactions: Clean and administer anti-allergy medications.
Facilitate Drainage: Aid drainage in conditions like blocked tear ducts.
Prevent Damage in Systemic Conditions: Monitor and manage complications in conditions like diabetes.
Educate Caregivers: Teach proper eye care techniques, signs of complications, and the importance of eye hygiene.
Purpose of Eye Medications
Topical medications are commonly used to treat eye diseases. They are administered to:
Treat Infections: Combat bacterial, viral, or fungal infections.
Manage Intraocular Conditions: Address diseases like glaucoma.
Prepare for and Aid Recovery from Surgery: Ensure optimal surgical outcomes.
Dilate Pupils: Facilitate eye examinations and refraction.
Provide Lubrication: Alleviate dryness and discomfort.

Care of the Child Undergoing Eye Surgery
Eye surgery for children encompasses pre-operative, intra-operative, and post-operative phases, each requiring meticulous care and attention.
Pre-operative Care
Conditions Necessitating Surgery: Common reasons for eye surgery in children include trauma, cataracts, foreign body removal, congenital malformations, glaucoma, eye injuries, astigmatism or strabismus, ptosis (drooping eyelid), and retinal detachment. The ophthalmologist will determine the appropriate treatment, which can range from a minor incision to enucleation (removal of the entire eyeball).
Admission: The child is admitted to a well-lit, clean bed in the pediatric surgical ward. The environment is kept free of dust to minimize infection risk.
History Taking: A detailed medical history is obtained, including previous surgeries, allergies, existing medical conditions, and current medications.
Physical Examination: A comprehensive physical exam assesses the child’s overall health, identifying potential risks. Vital signs (heart rate, blood pressure, temperature) are checked. The eyes are thoroughly examined to evaluate the specific condition and rule out other issues.
Observation: Continuous monitoring of vital signs (temperature, respiration, pulse, blood pressure) and the affected eye.
Investigations:
History: Gathering information from the child and parent.
Physical Eye Examination: Assessing the eye’s structure and function.
Tests: Visual acuity, visual field, and tonometry (measuring intraocular pressure to evaluate for glaucoma) may be performed.
Hospital Environment Orientation: Familiarizing the child with the hospital setting is crucial, especially if vision will be impaired post-surgery. Older children are helped to learn the layout of their room (furniture, doors, windows). Familiarization with voices and routine sounds is also beneficial.
Education: Comprehensive education regarding post-operative care and restrictions is provided. This includes keeping the head still, avoiding reading, showers, shampooing, tub baths, bending, heavy lifting, and sleeping on the operative side.
Diagnosis and Surgical Need Explanation: The diagnosis and rationale for surgery are clearly explained to the patient and family, addressing concerns and fears.
Reassurance and Counseling: Emotional support and reassurance are provided to alleviate anxiety. Counseling helps the patient cope with surgery-related stress.
Surgery Booking and Scheduling: The surgery date and time are scheduled, considering patient and surgical team availability. Patients are informed about actions to take if issues arise before the scheduled date.
One Week Prior to Surgery: Pre-operative tests and assessments (blood tests, imaging, specific exams) may be conducted. Medications or eye drops may be prescribed.
One Day Prior to Surgery: In some cases, temporary hospital admission may be required. Feeding and hygiene needs are addressed. A detailed history and physical exam, including ophthalmological tests, are performed. The patient is informed about personal requirements and procedural instructions.
Day of Operation:
Consent: The patient signs a consent form, agreeing to the procedure.
NPO (Nil Per Os): Depending on anesthesiologist instructions, the patient may need to refrain from eating or drinking for at least 8 hours before surgery.
Pre-Operative Care: Reassurance, hygiene measures, jewelry removal, and pre-medication administration (if necessary) are performed. Hydration may be provided as instructed.
Rest and Sleep: Ensuring adequate rest, minimizing noise, and reducing bright light exposure.
Physical Preparation:
Bowel Preparation: Bowel prep may be required to prevent straining post-surgery. This can involve a laxative or enema the night before.
Hair Removal: Eyebrow shaving, eyelash trimming, and facial shaving are performed only if ordered by the surgeon to ensure a sterile surgical field.
Post-Operative Bed Preparation: Depending on the surgery type, a post-operative bed with side rails and sandbags for head immobilization may be prepared for patient safety and to prevent accidental movement.
Transportation to Operating Room: Two nurses accompany the patient to the operating room for safety and support.
Post-operative Care:
Immediate Post-Operative Period
Retrieval from Operating Room: Upon the child’s return from surgery, nurses first check vital signs and obtain a comprehensive report from the surgical team to ensure continuity of care.
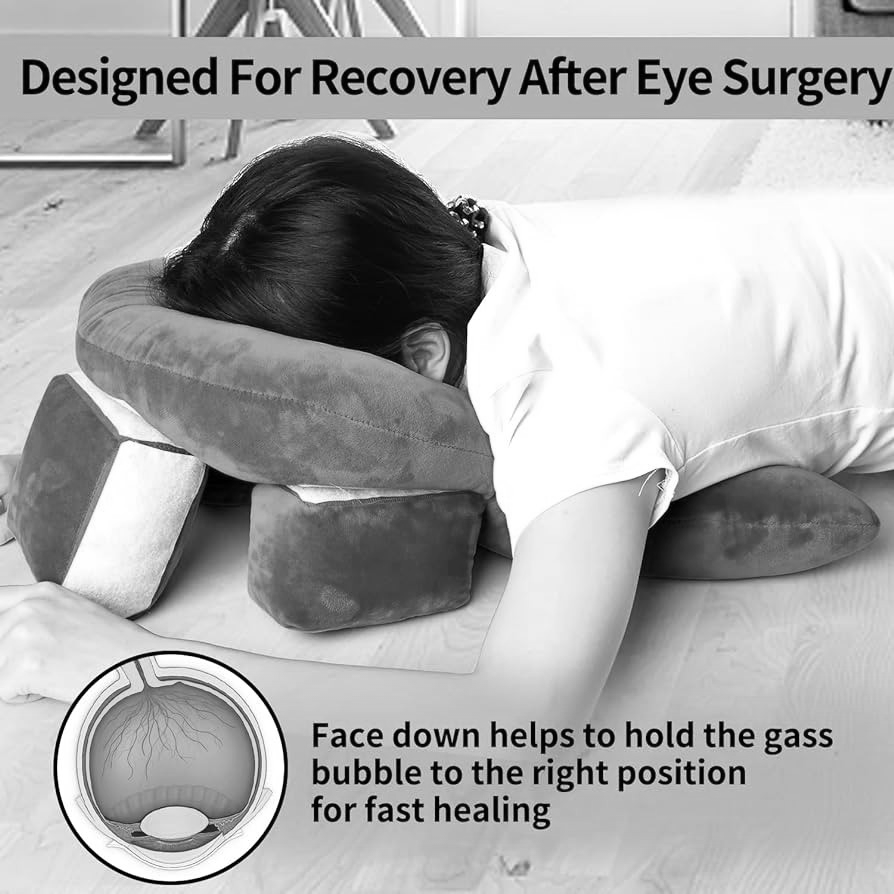
Transfer to Pediatric Surgical Ward: The child is transported in a post-operative bed, positioned face down as per the surgeon’s orders to optimize recovery and minimize complications.
Initial Care and Positioning in the Ward
Vital Signs Monitoring: Continuous monitoring of heart rate, blood pressure, respiratory rate, and oxygen saturation.
Positioning: Maintaining the prescribed face-down position for proper healing.
Immobilization: Using sandbags, if ordered, to immobilize the head and prevent movement that could hinder recovery.
Safety: Raising bed side rails if both eyes are bandaged to prevent falls. Ensuring the call bell is within easy reach.
Rest and Recovery
Anesthesia Recovery: Allowing the child to rest temporarily to recover from anesthesia effects.
Position Monitoring: Continuously ensuring the child maintains the surgeon-instructed position.
Ongoing Observations
Bleeding: Vigilant monitoring for any signs of bleeding from the surgical site.
Dressings: Regular checks to ensure dressings are secure, dry, and free from signs of infection or complications.
Welcoming the Child Back to the Ward
Reassurance: Providing comforting words and reassurance to ease anxiety upon waking.
Dressing Removal: Applying non-sterile gloves, removing old eye dressings/patches/shields, and discarding them appropriately. If dressings are stuck, moisten gauze with 0.9% NaCl solution and apply to the dressing.
Eye Assessment: Before proceeding, assess each eye and surrounding tissue for:
Redness
Swelling
Abrasions
Irritation (itching, stinging, burning)
Discharge (color, odor, volume)
Eyelid position (partial/full closure, blink)
If cooperative, ask the child to look up; if not, gently hold the child with parental help and pull the lower lid down.
If there’s encrustation on eyelids/lashes, dampen sterile gauze with 0.9% NaCl solution and apply.
If there’s discharge, perform an eye swab before cleansing.
Performing Eye Swabbing
Procedure: Use a sterile cotton wool swab to roll over the conjunctival sac inside the lower eyelid.
Specimen Handling: Place the swab in the transport medium and send it immediately to the laboratory.
Chlamydia Suspicion: Perform the eye swab after eye cleansing if Chlamydia infection is suspected.
Performing Eye Cleansing
Solution: Use 0.9% NaCl or sterile water in a sterile gallipot.
Technique: Moisten sterile gauze with the solution. Wipe the eye from the inner to the outer aspect, using a new gauze square for each stroke.
Infection Precaution: Clean the non-infected eye first.
Hand Hygiene: Decontaminate hands again after the procedure.
Instilling Eye Medication
Preparation: Cleanse the eye(s) before instilling medication.
Identification: Verify the child’s identification band against the medication prescription chart.
Consent: Adolescents over 16 can consent, but supervision is required if the medication affects vision.
Medication Containers: Use new medication containers post-surgery.
Procedure:
Gently place a hand on the forehead while holding the medication container.
Place a tissue/non-sterile gauze swab under the lower eyelid and gently pull down the lower eyelid.
Applying Eye Padding/Dressing(s)/Shields
Eye Padding: Apply gauze over the closed eyelid and secure it with tape.
Eye Dressings: Use polyacrylamide hydrogel dressings (Geliperm®) over the closed eyelid.
Eye Shield: Apply a clear shield over the affected eye and secure it with clear tape.
Precautions
Secure Dressings: Ensure eye dressings are secure with an eye shield or reinforce loose tape.
Restraints: Restrain the arms of children and disoriented patients as needed.
Positioning Monitoring: Continuously monitor sleeping patients to maintain proper positioning.
Avoid Jarring: Avoid jarring the bed to prevent startling the patient.
Emotional Monitoring: Monitor for depression or suicidal tendencies in newly blinded patients.
Oral Intake: Check physician’s orders before giving anything by mouth to prevent nausea/vomiting.
Approaching the Patient
Communication: Always speak to the patient upon entering their area and before touching them.
Explanation: Fully explain each procedure or activity.
Orientation: Reinforce orientation to surroundings.
Departure: Inform the patient when leaving their area.
Diversional Activity
Non-Fatiguing Activities: Provide non-fatiguing activities if eyes are not bandaged.
Visitors: Encourage visitors to chat or read to the patient.
Radio: Use a radio for entertainment and information.
Nursing Care of the Patient with Vision Loss
Physical Orientation: Describe the room and contents in detail; lead the patient around the room.
Precautions: Inform about room changes, keep doors fully open/closed, maintain toilet article placement, and remove hazards.
Assistance: Address the patient by name, inform them when leaving, and allow them to place their hand on your arm/shoulder when walking.
Independence: Encourage self-sufficiency.
Complications of Eye Surgery
Infections: Endophthalmitis (serious internal eye infection) can lead to vision loss if untreated.
Fluid and Swelling:
Cystoid Macular Edema: Swelling/fluid in the macula, causing blurred vision.
Corneal Edema: Swelling of the cornea, causing blurry vision and discomfort.
Bleeding: Hyphema (bleeding in the eye’s front chamber) causes pain, redness, and blurry vision.
Tissue Damage: Capsule rupture during surgery can lead to vitreous gel loss, causing blurry vision and other issues.
Retinal Detachment: The retina detaching from the underlying choroid can lead to permanent vision loss.
Cataract Formation: Rarely, eye surgery can trigger a new cataract.
Glaucoma: Eye surgery can sometimes increase intraocular pressure, potentially leading to glaucoma.
Dry Eye Disease: Dry eye can worsen or develop after surgery due to changes in the eye’s surface.
Care at Home After Eye Surgery
Bathing
Eyelid Cleaning: Clean eyelid edges at least twice daily with a moist, clean face cloth, avoiding pressure on the upper eyelid.
Showering/Bathing: Showering, tub baths, and hair washing are permitted the day after surgery.
Soap/Water Avoidance: Ensure no soap or water enters the eye for at least one week.
Eye Make-up: Avoid eye make-up for at least one week.
Fibrous Materials: Do not use cotton balls or make-up remover pads near the eye or under the eye shield.
Eye Care
Protective Eye Shield: Wear the shield when sleeping or lying down for at least one week to prevent accidental bumps or scratches.
Shield Cleaning: Clean the shield daily with 70% isopropyl alcohol and air dry before reusing.
Glasses: Wear old glasses if needed; vision may be better without them in the operated eye.
Shield Attachment: Attach tape to the forehead over the shield and tape it to the cheek.
Activity
Permissible Activities: TV, reading, and walks are allowed if tolerated.
Saunas/Hot Tubs: Avoid for at least one week.
Sleeping Position: Avoid sleeping on the operated side for at least two weeks.
Straining/Lifting: Avoid straining or lifting over 10 lbs (4.5 kg) for at least two weeks or until the surgeon advises otherwise.
Swimming/Submersion: Avoid swimming or head submersion for at least three weeks.
Strenuous Activities: Avoid strenuous activities or rough contact sports for at least four weeks or until cleared by the surgeon.
Eye Protection: Avoid rubbing or bumping the eye for at least six weeks.
Sexual Activity: Resume when comfortable.
Driving: Do not drive until cleared by the surgeon.
Healthy Eating
Diet: Resume regular diet post-surgery.
Constipation Prevention: Prevent constipation and straining by increasing fluids, activity, and fiber.
Medications
Regular Medications: Restart regular medications unless instructed otherwise by the doctor.
Postoperative Eye Drops: Obtain and take prescribed eye drops as directed.
Artificial Tears: Use artificial tears (e.g., Refresh™, Genteal™) for scratchiness, waiting 30 minutes after prescription drops.
When to Seek Help
Worsening Eyesight: If eyesight deteriorates.
Increasing Pain: If pain or ache in the eye increases.
Redness: If redness increases.
Swelling: If swelling around the eye occurs.
Discharge: If there is any discharge from the eye.
New Symptoms: If new floaters, light flashes, or field of vision changes occur.
How to Instill Eye Drops
Hand Washing: Wash hands before touching eye drops.
Head Tilt: Look at the ceiling from a sitting or lying position.
Pocket Formation: Use one or two fingers to gently pull down the lower eyelid, forming a pocket.
Drop Instillation: Keeping both eyes open, gently squeeze one drop into the pocket. Avoid the bottle top touching the eye, eyelashes, fingers, or any surface.
Eye Closure: Close the eye for 30-60 seconds for absorption.
Rubbing Avoidance: Do not rub the eyes; gently blot with a tissue if needed.
Multiple Drops: Wait about three minutes between different eye drops.

Responsibilities of Nurses in Ophthalmic Visual Acuity Testing
Visual acuity assessment, a measure of central vision sharpness, is fundamental in ophthalmic examinations. It evaluates the entire visual pathway, from the occipital cortex (brain) to the cornea (front of the eye), aiding in diagnosis and treatment planning. Nurses play a vital role in ensuring accurate and reliable testing.
Nurse’s Responsibilities
Patient Preparation:
Explanation: Clearly explain the test’s purpose and procedure to the patient.
Addressing Concerns: Answer any patient questions about the test.
Comfort: Ensure the patient is comfortable and relaxed, offering positioning assistance and support.
Language Barriers: Identify and address language barriers to ensure comprehension.
Test Performance:
Chart Selection: Choose the appropriate visual acuity chart based on age, literacy, and specific needs (e.g., Snellen for adults, LEA for children).
Distance: Ensure the correct patient-chart distance (typically 20 feet or 6 meters).
Occlusion: Properly cover the non-tested eye to prevent cross-viewing.
Recording: Accurately document visual acuity for each eye, including distance and line identified.
- Identifying Factors Affecting Acuity:
Refractive Error: Assess for signs of refractive errors (nearsightedness, farsightedness, astigmatism) that could impact acuity.
Media Opacity: Observe for cloudiness in the ocular media (cornea, lens, vitreous) that could interfere with light transmission.
Patient Cooperation: Note any lack of cooperation or comprehension affecting test accuracy.
Reporting Observations:
Communication: Communicate relevant observations (cooperation, suspected refractive errors, media opacity signs) to the ophthalmologist for further evaluation.
Factors Influencing Accurate Visual Acuity Testing
Patient Cooperation: Patient must understand and follow instructions, focusing on the chart and maintaining a fixed gaze.
Form Recognition: Patient must be able to identify forms on the chart.
Ocular Media Clarity: Cornea, lens, and vitreous must be clear for light to pass through.
Focusing Ability: The eye must be able to focus properly on the chart.
Eye Convergence: Both eyes must work together to converge on the target.
Retinal Function: The retina must be able to receive and process visual information.
Intact Visual Pathways: The optic nerve and brain pathways must be intact for visual information transmission.
Common Charts for Distance Visual Acuity Measurement
Snellen Chart: Most common for literate adults. Distance vision is tested at 6 meters. If the patient wears glasses, vision may be recorded with and without them, noting it on the record. Each eye is tested separately, with the other covered.
Description: Features black letters, numbers, or symbols on a white background, arranged in nine rows of decreasing size. The top letter is readable by a normal eye at 60 meters; subsequent rows are readable at 36, 24, 18, 12, 9, 6, 5, and 4 meters, respectively.
Procedure:
One eye is tested at a time, the other covered.
The patient reads lines from top to bottom.
The smallest readable line indicates visual acuity.
Recording: Visual acuity is recorded as a fraction (e.g., 20/20, 6/6), where the numerator is the patient’s reading distance and the denominator is the distance a person with normal vision can read that line.
Pinhole Testing:
Purpose: Used when visual acuity is below average to determine if the cause is refractive error (uncorrected by glasses) or another condition.
Method: A pinhole disc allows only central light rays to reach the macula, reducing blur from refractive errors. A pinhole disc is used if the VA is less than 6/6 or 6/9.
Interpretation:
Significant improvement with pinhole suggests refractive error.
No improvement suggests another underlying condition.
Sheridan Gardner Test Chart: Used for children and illiterate patients.
Description: Features a single reversible letter (e.g., A, V, N) on each line. The child holds a card with these letters.
Procedure:
The patient holds a card with the same letters.
The examiner points to a letter on the chart.
The patient points to the corresponding letter on their card.
Kay Picture Chart: Used for illiterate patients or children.
Description: Contains pictures of varying sizes instead of letters.
Procedure: The patient identifies the pictures. An interpreter may be needed for patients with language difficulties.
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowRelated Topics
Specialized Nursing Care Procedures
- Perform Shortening and removal of drains
- Perform Colostomy Care
- Prepare Abdominis Paracentesis (Abdominal Tapping)
- Prepare Lumbar Puncture
- Perform Gastrostomy Feeding
- Carry out gastric Lavage
- Perform Tracheostomy Care
- Ophthalmological Care
- Care of the patient`s ears
- Pre-Operative Eye Care
- Ear Care
- Peri-Operative Care:
- Orthopedic Nursing Care
- Prepare for Neurological Assessment
We are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved