Obstetric Anatomy and Physiology
Varieties of Pelvis (Caldwell-Moloy Classification)
Table of Contents
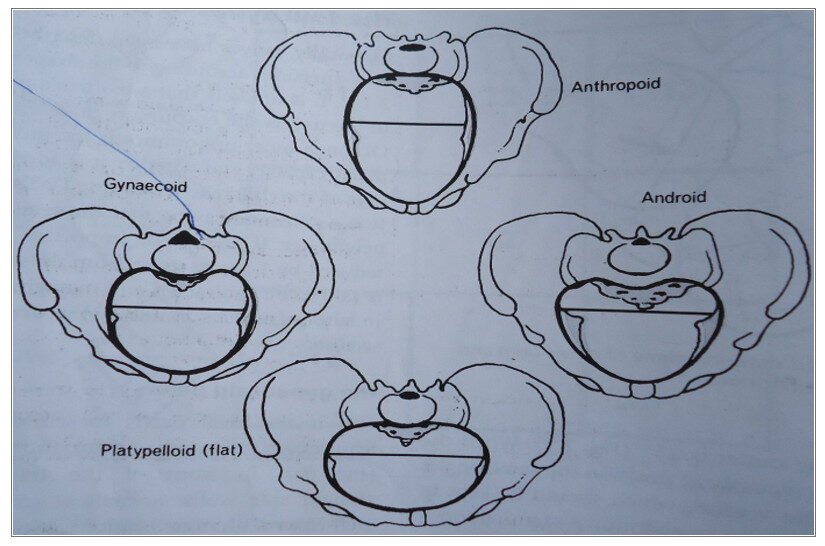
TYPES OF PELVIS
It’s possible to tell the sex and race by the shape of the pelvis. There are four main types of the pelvis:
(1) Gynaecoid
(2) Android
(3) Platypelloid
(4) Anthropoid
(5) Others:
- Robert’s pelvis
- Naegele pelvis
- Justo minor pelvis
- Contracted pelvis
GYNAECOID
This is another name for normal female pelvis which is:
- The brim: Is normal shape.
- Fore pelvis is generous.
- Side walls are straight, sacrum well curved, cavity shallow, sciatic notches rounded.
- Has well rounded ischial spines.
- The outlet: Has well round angle, 90 degrees and accommodates 2½ fingers. Incidence: 50% of general population.
EFFECTS ON LABOUR
The fetus presents by vertex with the occiput anterior crowning part of the head, which is the most favorable position of the onset of labor. Therefore a normal vaginal delivery is expected.
ANDROID PELVIS
This is a male type of pelvis. The bones are heavier than the gynaecoid pelvis.
- The brim is heart shape making the pelvis very narrow.
- The transverse diameter does not cross the center of the pelvis, but is much nearer to the sacrum.
- There is more space at the back than the front. (Fore pelvis is narrow)
- The cavity of the hollow of the sacrum has a poor curved (straight sacrum). The sacrum is large giving a deep tunnel shaped cavity. The greater sciatic notch is narrow.
- The outlet, the pubic arch is sharp, reducing the available space, subpubic angle is less than 90 degrees, the ischial spines are sharp and turning inwards leading to reduced transverse diameter. Incidence: 20% of the general population. Commonly found in short, heavily built women who have a tendency of being hairy.
EFFECTS ON LABOUR
The fetus presents with occiput lying posterior where there is more room. It may pass the brim and cavity but may be obstructed at the outlet due to prominent ischial spines, instrumental delivery becomes necessary.
PLATYPELLOID PELVIS
May be due to rickets, the brim has a short anteroposterior diameter lengthened – transverse diameter giving a kidney shaped appearance (bean shaped).
- The cavity: The diameter is affected as the brim but there is more room for the fetal head.
- The outlet: The pelvis is shallow, there is a wide subpubic arch giving adequate outlet (also include flat pelvis).
THE FOUR TYPES OF PELVIS
EFFECTS ON LABOUR
Fetal head finds difficult in engaging in the pelvis or presents with the long diameter of the head across the transverse diameter where there is room leading to:
- With good contractions, the fetal head is pushed to and fro between the sacral promontory and symphysis pubis therefore it rocks and rolls through the brim and cavity. The skull bones overlap each other and the process known as asynclitism.
- The fetal head may be obstructed in the narrow diameter of the brim and uterine contractions cause the head to extend as it descends leading to false presentation.
- If the brim is greatly contracted the fetal head remains high above leading to caesarean section.
ANTHROPOID PELVIS
Found in very tall, long legged women, common in S. Africa.
- The brim is oval shaped having a long anteroposterior diameter but a reduced transverse, fore pelvis narrowed.
- The cavity is adequate in all diameters but rather deep.
- The outlet is adequate in all diameters with a wide pubic arch.
EFFECTS ON LABOUR
The fetus presents with a long diameter of the head in the anteroposterior diameter, the occiput lying in the hollow of the sacrum resulting in face to pubis delivery instead of face to perineum.
OTHER PELVIC VARIATIONS
JUSTO MINOR PELVIS
Is a small gynaecoid pelvis but the diameters are reduced found in small women less than 1.5 m tall. The type of delivery depends on the size of the husband and fetus she may deliver a small baby vaginally with very little trouble. On the other hand, a larger baby may require a forceps delivery or even caesarean section.
CONTRACTED PELVIS
The essential diameters are reduced by 1 cm or more i.e. anteroposterior, oblique or transverse of brim, cavity or outlet is reduced by 1 cm or more.
HIGH ASSIMILATION PELVIS
This occurs when the 5th lumbar vertebra is fused to the sacrum (made up of 6 vertebrae) and the angle of inclination of the pelvic brim is increased. Engagement of the head is difficult but once achieved labor progress normally.
LOW ASSIMILATION PELVIS This is made up of 4 sacral vertebrae.
DEFORMED PELVIS This may occur from developmental anomalies or dietary deficiencies, injury or disease.
Examples of developmental anomalies of the pelvis:
ROBERT’S PELVIS
The pelvis has no wings (ala) of the sacrum contracted in all its diameter (rarely seen) its due to congenital abnormality caesarean section is done.
NAEGELE PELVIS
Only one wing is present in the sacrum giving it an obliquity of the pelvis, may be due to congenital abnormality, sometimes caused by injury. It’s rare but can occur in a woman who has walked with a limp for many years can be delivered by caesarean section.
DIETARY DEFICIENCY PELVES INCLUDE: Deficiency of vitamin and minerals necessary for the formation of health bones may complicate labor to some extent.
OSTEOMALACIC PELVIS The disease osteomalacia is rare. It’s due to deficiency of calcium and occurs in adults. As bones of the skeleton soften due to the gross calcium deficiency, the pelvic canal is flattened together until they become Y shaped slit. Labor is impossible caesarean section would be performed in early pregnancy incarceration of the gravid uterus may occur because of the gross deformity.
RACHITIC PELVIS
Rickets in early childhood can lead to gross deformity of pelvic brim. The weight of the upper body presses downwards on to the softened pelvic bones. The sacral promontory is pushed downwards and forward, and the ilium and ischium are down outwards. These results in a flat pelvic brim like that of the platypelloid pelvis. The sacrum tends to be straight with the coccyx bending accurately downwards. The tuberosities are wide and the pubic arch is wide. (1) Bow legs (2) Spinal deformity
OUTCOME OF LABOUR
If severe contractions are present caesarean section is performed. The fetal head enters the pelvis by lateral fitting of the head known as asynclitism.
ANTERIOR ASYNCLITISM
The anterior bone moves downward behind the symphysis pubis until the parietal eminence enters the brim. The movement is then reversed with the head tilts in the opposite direction until the posterior parietal bone negotiates the sacral promontory and the head is engaged.
POSTERIOR ASYNCLITISM
The movements of anterior asynclitism are reversed; the posterior parietal bone negotiates the sacral promontory prior to the anterior parietal bone moving downwards behind the symphysis pubis. Once the fetal head has engaged, descent progresses normally accompanied by flexion and internal rotation. Labor may be completed by face, brow presentation and cord prolapse.
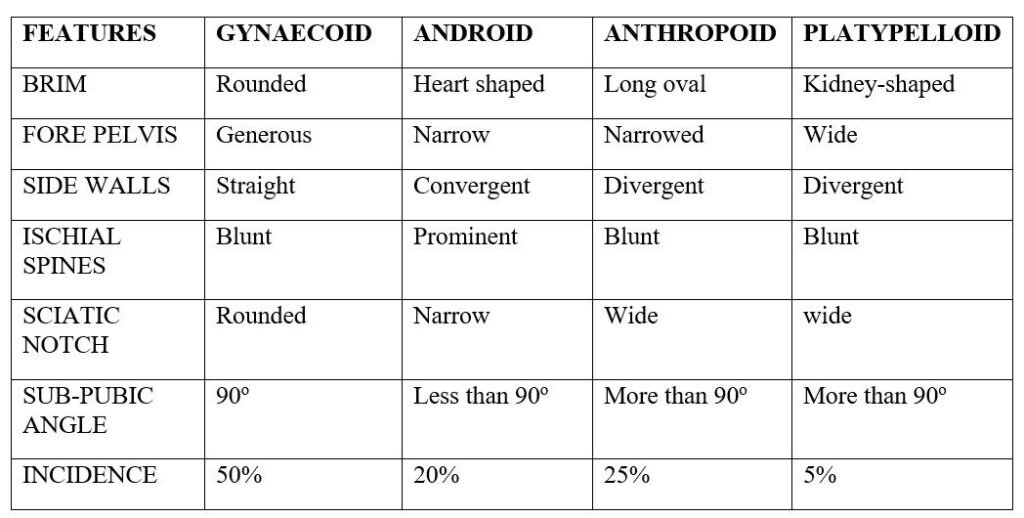
SUMMARY OF FEATURES OF THE FOUR TYPES OF PELVIS
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowWe are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved