Tropical Diseases
Schistosomiasis
Table of Contents
Definition
Schistosomiasis (also known as bilharzia or snail fever) is a disease of the large intestine and urinary tract caused by parasitic worms of the Schistosoma blood fluke. It may infect the urinary tract or intestines.
Cause
- Schistosoma haematobium causes urinary schistosomiasis.
- Schistosoma mansoni and Schistosoma intercalatum cause intestinal schistosomiasis.
- Schistosoma japonicum and Schistosoma mekongi cause Asian intestinal schistosomiasis.
- Avian schistosomiasis species cause swimmer’s itch.
Causal Agents
Schistosomiasis (Bilharziasis) is caused by some species of blood trematodes (flukes) in the genus Schistosoma. The three main species infecting humans are Schistosoma haematobium, S. japonicum, and S. mansoni. Three other species, more localized geographically, are S. mekongi, S. intercalatum, and S. guineensis (previously considered synonymous with S. intercalatum). There have also been a few reports of hybrid schistosomes of cattle origin (S. haematobium x S. bovis, x S. curassoni, x S. mattheei) infecting humans. Unlike other trematodes, which are hermaphroditic, Schistosoma spp. are dioecous (individuals of separate sexes).
Transmission
The disease is spread by contact with water that contains the parasites. These parasites are released from freshwater snails that have been infected. The larvae form (cercariae) of schistosoma penetrates the skin from contaminated water.
Epidemiology
Schistosomiasis affects almost 210 million people worldwide. An estimated 12,000 to 200,000 people die from it a year. The disease is most commonly found in Africa, Asia and South America. Around 700 million people, in more than 70 countries, live in areas where the disease is common. Schistosomiasis is second only to malaria, as a parasitic disease with the greatest impact.
Life Cycle
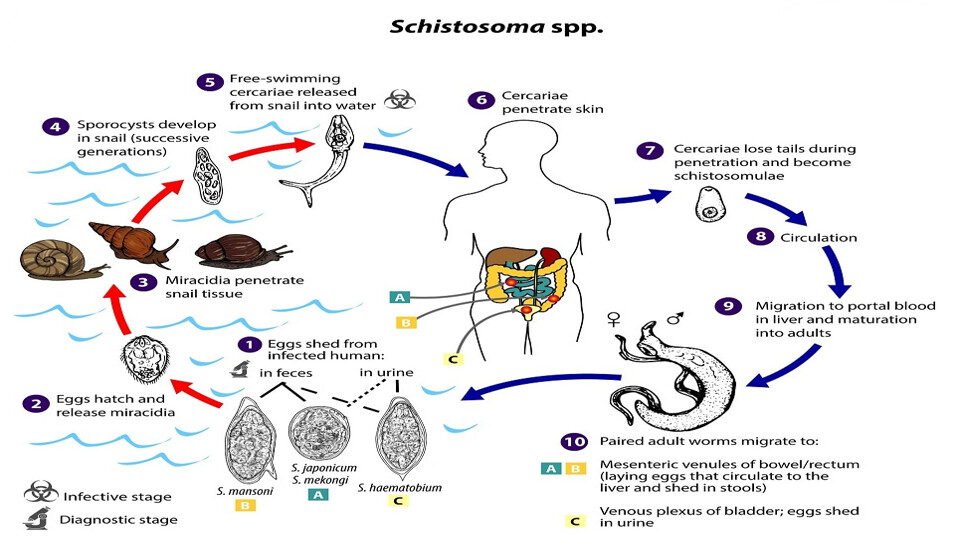
- Schistosoma eggs are eliminated with feces or urine, depending on species.
- Under appropriate conditions the eggs hatch and release miracidia, which swim and penetrate specific snail intermediate hosts.
- The stages in the snail include two generations of sporocysts and the production of cercariae.
- Upon release from the snail, the infective cercariae swim, penetrate the skin of the human host, and shed their forked tails, becoming schistosomulae.
- The schistosomulae migrate via venous circulation to lungs, then to the heart, and then develop in the liver, exiting the liver via the portal vein system when mature.
- Male and female adult worms copulate and reside in the mesenteric venules, the location of which varies by species (with some exceptions).
Species-Specific Locations
- S. japonicum is more frequently found in the superior mesenteric veins draining the small intestine.
- S. mansoni occurs more often in the inferior mesenteric veins draining the large intestine.
- However, both species can occupy either location and are capable of moving between sites.
- S. intercalatum and S. guineensis also inhabit the inferior mesenteric plexus but lower in the bowel than S. mansoni.
- S. haematobium most often inhabits in the vesicular and pelvic venous plexus of the bladder, but it can also be found in the rectal venules.
- The females (size ranges from 7–28 mm, depending on species) deposit eggs in the small venules of the portal and perivesical systems.
- The eggs are moved progressively toward the lumen of the intestine (S. mansoni, S. japonicum, S. mekongi, S. intercalatum/guineensis) and of the bladder and ureters (S. haematobium), and are eliminated with feces or urine, respectively.
Signs and Symptoms
Above all, schistosomiasis is a chronic disease.
Schistosoma haematobium (Urinary Tract)
- Painless blood stained urine at the end of urination (haematuria)
- Frequency of urination (cystitis and fibrosis)
- Hydronephrosis, pyonephrosis, hypertension, uraemia.
- Fatigue
- Genital sores
Schistosoma mansoni (GIT)
- Abdominal pain
- Frequent stool with blood stained mucous
- Palpable liver (hepatomegaly)
- Haematemesis
- Cough
- Diarrhea
- Fever
- Fatigue
Other Symptoms
- Skin symptoms: At the start of infection, mild itching and a papular dermatitis of the feet and other parts after swimming in polluted streams containing cercariae.
Diagnosis
- History of staying in an endemic area.
- Urine examination (for Schistosoma haematobium ova)
- Stool examination (for Schistosoma mansoni ova)
- Bladder x-ray for calcification or Ultrasound for urinary tract
- Cystoscopy.
- Detection of parasitic antigens by ELISA (blood sample).
- Tissue biopsy: (rectal biopsy (snip) for all species and biopsy of the bladder for S. haematobium) may demonstrate eggs when stool or urine examinations are negative.
Treatment
Schistosomiasis is readily treated using a single oral dose of the drug Praziquantel annually, (40mg/kg).
Prevention
- Avoid defecating or urinating in or near water
- Avoid washing or stepping in contaminated water
- Effective treatment of cases
- When a village reports more than 50 percent of children have blood in their urine, everyone in the village receives treatment.
- Clear bushes around landing sites
- Eliminating the water-dwelling snails that are the natural reservoir of the disease. Copper sulfate and Niclosamide can be used for this purpose.
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowWe are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved