Specialized Nursing Care
Subtopic:
Nasogastric tube to feed patients
Table of Contents
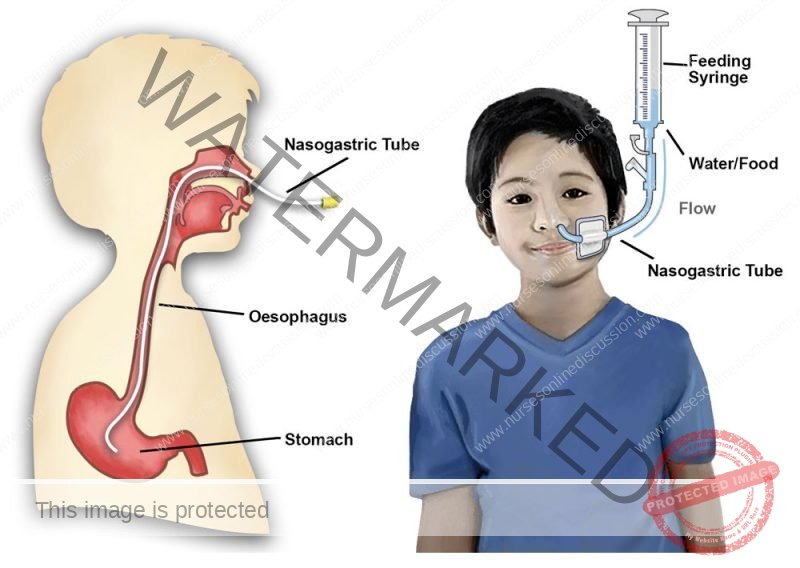
Naso-Gastric Tube and Tube Feeding
Indications for Naso-Gastric Tube Insertion
Insertion of a naso-gastric (NG) tube is indicated in the following situations:
Unconscious patients – Unable to swallow.
Post-operative patients – Especially after surgery involving the mouth, pharynx, or larynx.
Oesophageal obstruction/stricture – Due to inflammation or tumours.
Severe dysphagia – Patients with extreme difficulty in swallowing.
Neonates/infants – Who are too weak to suck or feed orally.
Severely burned patients – Due to increased metabolic needs and/or inability to feed orally.
Mentally ill patients – Who are unable or unwilling to eat.
Persistent nausea and vomiting – For gastric decompression or nutritional support.
Gastric lavage – For cleaning or washing out the stomach.
Collection of gastric specimens – For diagnostic purposes.
Equipment Checklist for NG Tube Insertion
A. On the Trolley (Top Shelf)
Sterile NG tubes (appropriate size) in a bowl
Warm water (to soften the tube)
Gallipot with gauze swabs
Orange sticks or nasal speculum (for nostril inspection)
Receiver/kidney dish with blue litmus paper (to test tube placement)
Mackintosh cape and towel/dressing mackintosh
10 ml syringe (to check air or aspirate content)
Spigot or clamp (to close the tube after insertion)
Cup of water (to rinse patient’s mouth)
Vomit bowl (kidney dish)
Strapping/adhesive tape (to secure tube to the nose)
Receiver (for used swabs and other waste)
B. At the Bedside
🧼 Hand hygiene supplies (sink, soap, water, towel)
🛑 Screens or curtains (to ensure patient privacy)
🩺 Stethoscope (to confirm placement)
📋 Patient’s chart (to verify doctor’s order and for documentation)
🗑️ Waste receptacle (for disposal of used materials)
Procedure (Passing Naso-Gastric Tube)
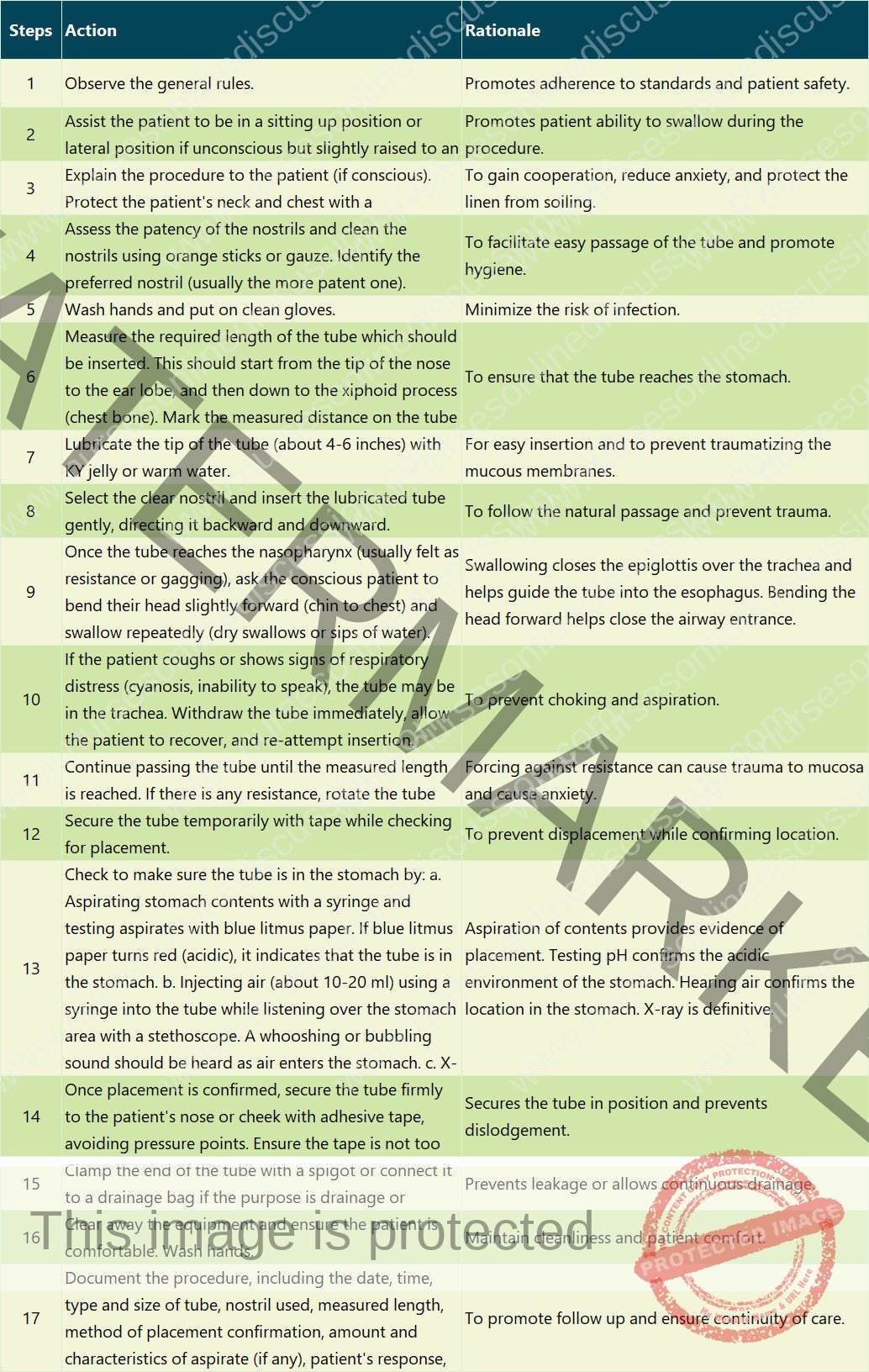
Points to Remember (Passing NG Tube):
- Never force the tube if resistance is met.
- Listen carefully for signs of respiratory distress during insertion.
- Always verify tube placement before administering anything through the tube.
- Change the tube as per policy or doctor’s prescription (often weekly).
- Ensure a communication system (e.g., pen and paper, bell) is available for the patient if they cannot speak.
Naso-gastric feeding can be given in two ways:
- Intermittent feeding: Given at intervals as ordered by the doctor (e.g., four hourly).
- Continuous drip: Given as a continuous infusion over a specified period (e.g., 24-hour period).
Requirements (Feeding)
Trolley:
- Prepared feed (correct type, amount, and temperature)
- A feed bowl of warm water (if feed needs warming)
- A cup with warm water (for rinsing the tube)
- A 50 ml syringe barrel or a funnel with tubing and connection (appropriate for the tube)
- Vomit bowl (kidney dish)
- Mackintosh cape and towel /dressing mackintosh
- Stethoscope (for checking placement)
- Spigot or clamp
- Patient’s chart
- Waste receptacle
Bedside:
- Hand washing equipment
- Screens (for privacy)
Procedure (Feeding):
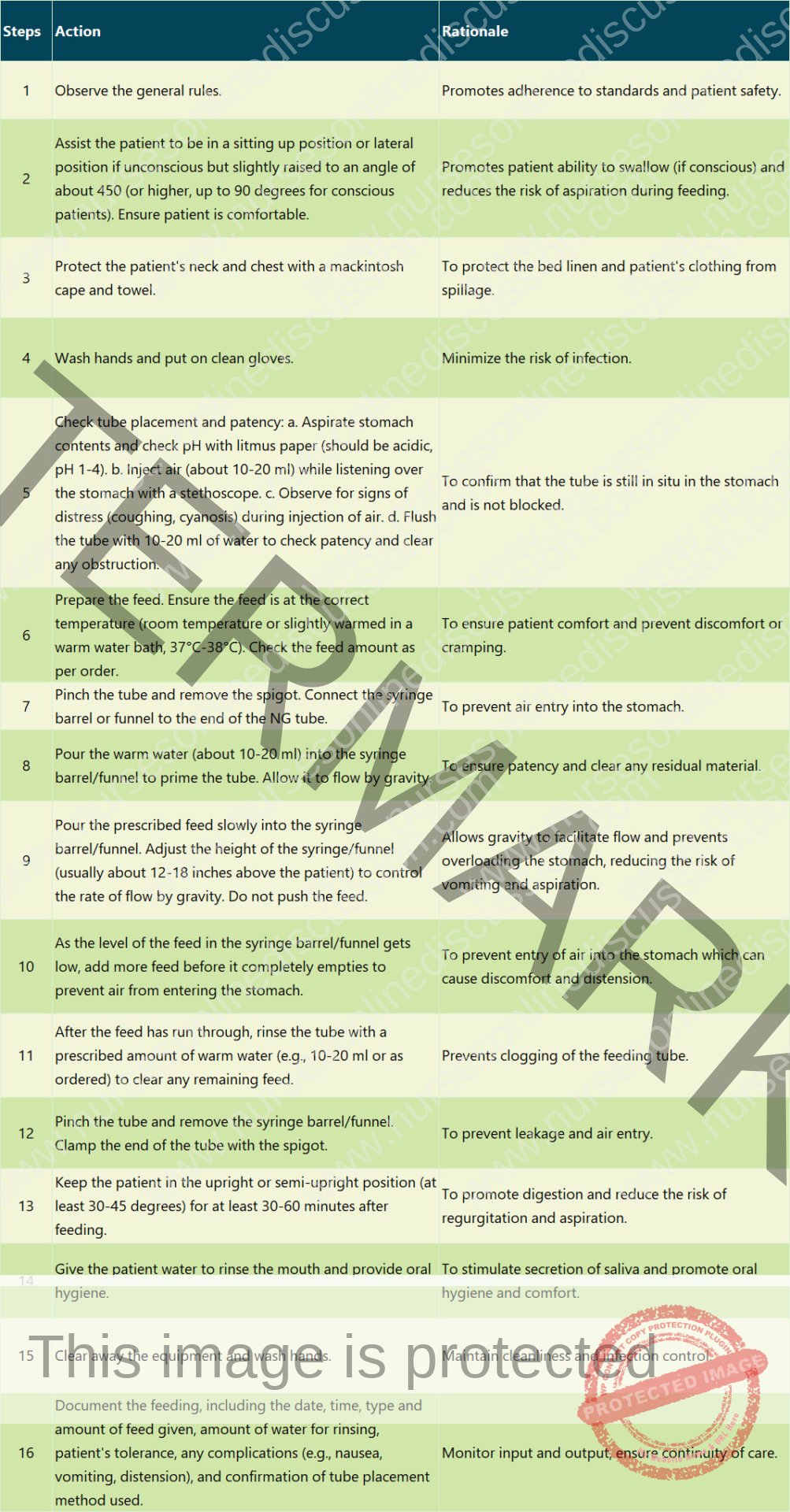
Points to Note (Feeding)
- Always verify tube placement before each feeding or medication administration.
- Never push feeds into the tube using the plunger of the syringe; allow gravity to control the flow rate.
- Keep the patient in a semi-Fowler’s or Fowler’s position during and after feeding.
- Monitor the patient for signs of intolerance such as nausea, vomiting, abdominal distension, diarrhea, or coughing.
Related Topics
- Wound dressing
- Colostomy Care
- Abdominal Paracentesis(Abdominal Tapping)
- Vulva Toilet/ Swabbing
- Oxygen Administration
- Lumbar Puncture
- Nasogastric tube to feed patients
- Gastrostomy Feeding
- Gastric Lavage
- Catheterization
- Tracheostomy Care
- Caring for patients in traction
- Prepare for application of orthopaedic splints
- Bandaging
- Nursing Process
- Take History of the patient
- Perform a physical examination of the Patient
- Making a Nursing Care Plan
- Admission of a patient
- Drug administration
- Transfer Patients
- Discharge of patients
- Last Office
We are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved