Specialized Nursing Care
Subtopic:
Nursing Process
The Nursing Process
Definition
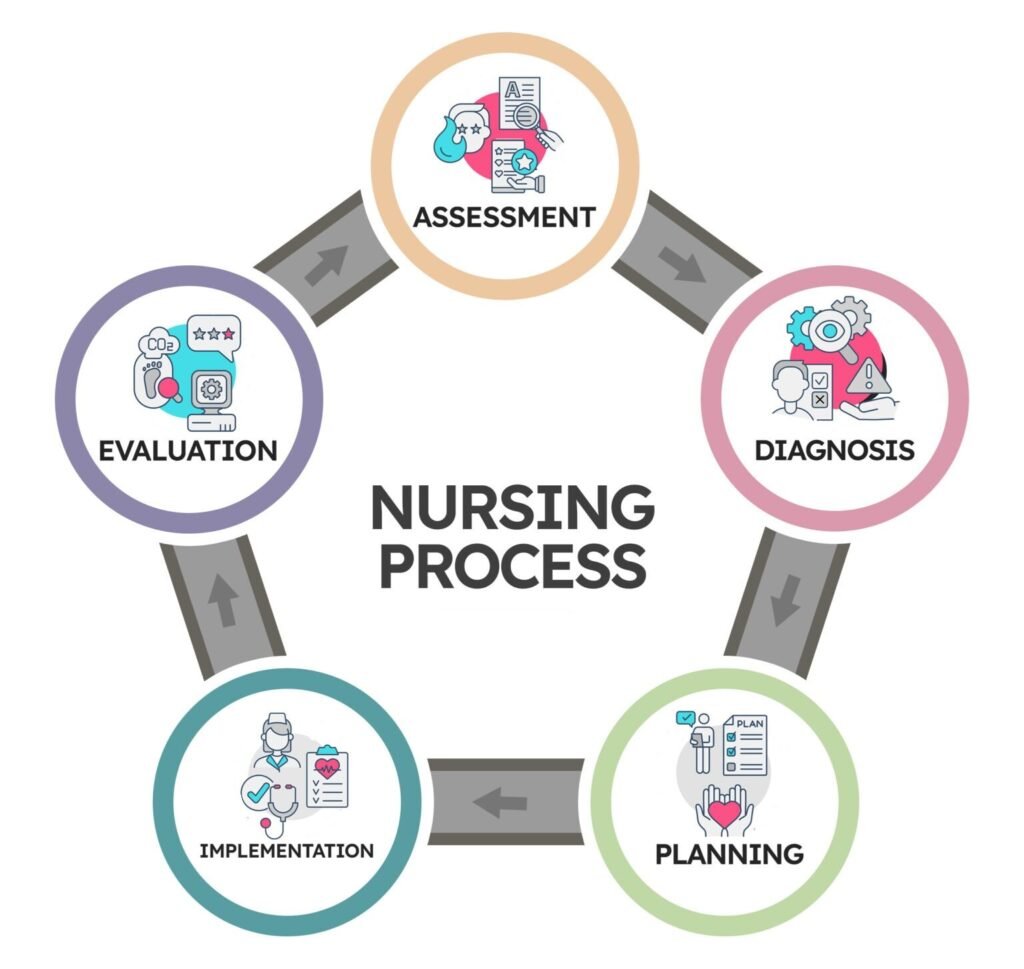
The nursing process is defined as a systematic, organized, dynamic, and methodical approach focused on identifying and treating the unique responses of individuals or groups to actual or potential alterations in health.
It involves five main phases:
Assessment
Nursing Diagnosis
Planning
Implementation
Evaluation
Characteristics of the Nursing Process
It must be planned systematically.
It must be patient-centered.
It must be patient/client oriented.
It must be goal-directed.
It must be outcome-oriented.
Key Questions in the Nursing Process
The process involves answering the following questions:
What is wrong with this patient?
What are this patient’s needs?
What can be done to help the patient?
Which planned nursing actions will help this patient?
How will the planned nursing actions be implemented and why?
Were the solutions effective? What were the results of nursing care?
3.1 Health Assessment
Definition
Assessment is the first phase of the nursing process. It includes gathering information (data) about a patient’s or client’s health status to identify actual or potential health problems.
Components of Assessment
Data Collection
Data Organization and Validation
Data Analysis
(i) Data Collection
Involves gathering information to create a patient database. Data is categorized into:
Subjective Data: Information obtained directly from the patient through interviews (e.g., symptoms).
Objective Data: Information obtained independently by the nurse or health team through observation, physical exams, or diagnostic tests.
Sources of Data
The patient (primary source)
Family members and significant others
Patient records
Health team members
Methods of Data Collection
Observation
Interview
Physical Examination
Nursing History
Differs from medical history.
Focuses on identifying existing and potential problems to form a base for nursing care planning, implementation, and evaluation.
Should avoid duplicating data already found in medical histories.
Can use a checklist format, covering content areas and classifications of patient conditions.
Assessment Equipment
Trolley Setup
Top Shelf (Observation Tray):
Thermometer
Watch
Stethoscope
Blood pressure machine
Neurological Tray:
Torchlight
Pen-light
Spatula
Patella hammer
Other Tools:
Ophthalmoscope
Tuning fork
Gallipot with cotton swabs/gauzes
Skin pencil
Snellen’s chart
Auroscope & Auroscope eye drop
Addison Horning probe
Blood & applicators
Dissecting forceps
Sterile throat swab
Dental mirror
Laryngoscope
Nasal speculum
Ear swabs
Lubricant
Drip
Vaginal speculum
Disposable pads
Bottom Shelf:
Record forms
Disposable gloves
Specimen bottles
Side Items:
Weight scale
Privacy screen
Examination table
Hand washing equipment
Special Senses Equipment
Bottles for cold and hot water
Bottles with distinctive smelling liquids (e.g., lavender)
Bottles with salt, sugar, bitter, and sour substances
Taking History of the Patient
Procedure:
Step 1: Follow General Rules for Procedure
Rationale: To maintain professional standards.
Step 2: Take the History in the Following Order
Biographical/Personal Information
- Name
- Age
- Tribe
- Address
- Occupation
- Religion
- Marital status
- Level of education
- Telephone number
- Patient or nearest of kin
Rationale: For identification, legal purposes, follow-up, and to create a therapeutic relationship.
Step 3:Presenting or Main Complaint
- Reason for seeking healthcare
- Onset: When did it begin?
- Has it gotten better, worse, or remained the same?
Rationale: Helps the nurse understand the patient’s main concern and form the basis for the nursing care plan.
Symptom Analysis
- Character: How does it feel, look, smell, sound? Severity?
- Anatomical location: Where is it located? Does it radiate anywhere?
- Duration: How long does it last? Does it recur?
- Setting: In what context does it occur?
- Pattern/Precipitating Factors: What makes it better or worse?
- Associated Symptoms: Any other symptoms occurring alongside?
Step 4: Social History
- Alcohol and tobacco use
- Source of income
- Housing and environmental conditions
- Source of water
- Marital status
- Number of children
- Health of spouse and children
- Recreational activities and entertainment
- Sexual activity, sex partners, family planning
Rationale: Identifies risk factors or conditions linked to lifestyle and social context.
Step 5: Family History
- Parents: Alive or deceased? Cause of death?
- Spouse: Health condition
- Children: Age and illnesses
Rationale: Helps to identify hereditary issues and general wellbeing of the household.
Step 5: Medical History
- Past illnesses or recurring conditions:
e.g., sickle cell, asthma, malaria, kidney disease, diabetes, STIs, poliomyelitis, rickets - Past hospitalizations or acute infections
Rationale: Assists in identifying underlying health issues affecting the current condition.
Step 6: Surgical History
- Past accidents or injuries
- History of blood transfusions (reason and outcome)
- Any fractures
Rationale: Establishes any lasting effects or complications from prior treatments or procedures.
Step 7: Past Medications
- Previous medications taken and patient’s response
- Any current medications?
- Allergies
- Use of home remedies or herbal medicines
Rationale: Prevents drug interactions and supports safe care planning.
Step 8: Gynecological History (for female patients)
- Menarche (age at first menstruation)
- Menstrual cycle details: length, flow, regularity
- History of STIs
- Tumors, cervical/uterine cancer
- Cysts, abortions, abnormal discharges
Rationale: Rules out gender-specific diseases and reproductive health issues.
Step 9: Male History (for male patients)
- Fertility-related conditions
- Sexually transmitted infections or conditions
Rationale: Identifies male reproductive and sexual health concerns.
Taking Height and Weight
Objectives:
- Identify requirements for taking height and weight.
- Prepare equipment for weight and height measurement.
- Perform accurate assessment of height and weight.
Requirements
Tray:
- Measuring tape
- Ruler
- Record chart
Bedside:
- Weighing scale (electronic or sling)
- Measuring pole
Procedure
| Step | Action | Rationale |
|---|---|---|
| 1 | Check patient’s weight using an electronic scale. | |
| 2 | Assess patient’s ability to stand on a weighing scale. | Ensures safety of the patient. |
| 3 | Wash hands. | Reduces transmission of organisms. |
| 4 | Explain the procedure and ask patient to pass urine. | Helps gain cooperation; empty bladder for accurate weight. |
| 5 | Ask patient to remove shoes and heavy clothing; wear hospital gown. | Extra clothing may cause errors in weight reading. |
| 6 | Place the weighing scale close to the patient. | Reduces risk of fall or injury. |
| 7 | Turn on and calibrate scale to zero. | Ensures accurate reading. |
| 8 | Instruct patient not to step on scale until display shows zero. | Prevents premature measurement. |
| 9 | Ask patient to stand straight and still. | Ensures accurate reading. |
| 10 | Read weight after digital numbers stabilize. | Weight is inaccurate if numbers are fluctuating. |
| 11 | Assist patient off the scale back to bed or wheelchair. | Reduces risk of injury. |
| 12 | Wash hands. | Maintains infection prevention. |
| 13 | Record the procedure. | Documentation for care continuity. |
Height Measurement
| Step | Action | Rationale |
| 14 | Ask patient to remove shoes. | Ensures accurate height measurement. |
| 15 | Secure or hold measuring tape vertically on the wall. | |
| 16 | Measure height using a wall-mounted device or measuring pole. | Obtains accurate height. |
| 17 | Instruct patient to stand straight with heels together. | Proper posture for accuracy. |
| 18 | Place ruler horizontally at 90° to tape; read height in cm/inches. | Correct positioning ensures accuracy. |
| 19 | Guide patient back to a comfortable bed position. | Ensures patient comfort. |
| 20 | Wash hands and record the procedure. | Promotes infection control and care continuity. |
| 21 | Clear equipment and reassure patient. | Concludes procedure with patient-centered care. |
Physical Examination
Definition: Physical examination of a patient involves a systematic head-to-toe assessment, including evaluation of the major body systems.
Techniques of Physical Examination
Inspection
Careful visual observation of the patient to identify signs of illness.Palpation
Using hands to touch and feel the body. Different hand parts provide different sensations:
- Fingertips: fine tactile discrimination.
- Back of fingers: temperature.
- Flat of palm and fingers: vibrations.
Percussion
Determines body density through sound produced when body parts are tapped. Helps identify:Solid masses, fluid, or gas.
Size and borders of organs (e.g., heart).
Steps in Percussion:
- Place middle finger of the left hand on the target area.
- Tap the end joint of this finger with the middle finger of the right hand.
- Apply 2–3 taps per area.
- Compare sounds in different regions.
Auscultation
Listening to body sounds using a stethoscope (e.g., heart, lung, and bowel sounds).
Functional Health Pattern Approach
Based on Gordon’s functional health patterns, this approach collects comprehensive data across 11 domains:
- Health perception/health management
- Nutritional/metabolic
- Elimination
- Activity/exercise
- Sleep/rest
- Cognitive/perceptual
- Self-perception/self-concept
- Role/relationship
- Sexuality/reproductive
- Coping/stress tolerance
- Value/belief
Data Grouping
Organizing collected data into relevant categories (functional health patterns) to:
- Identify patient strengths and problem areas.
- Detect missing or inconsistent information.
Data Analysis
After data collection, the nurse critically examines the findings and compares them to normal standards. Conclusions may include:
- No problem identified.
- Potential problem.
- Actual problem.
- Wellness diagnosis.
Examples:
- Potential problem: A patient on traction may develop pressure sores.
- Actual problem: A postoperative patient is actively bleeding.
General Physical Examination
Procedure:
Observe general rules of nursing procedures.
Observe general appearance – posture, gait, movement, hygiene.
Rationale: To identify obvious changes.
Inspection
Inspect the patient’s general condition.
Observe the patient’s ability to respond to verbal commands.
Rationale: Indicates speech and cognitive function.Observe the patient’s level of consciousness and orientation.
Rationale: Indicates brain function.Observe the patient’s ability to think, remember, process information, and communicate.
Rationale: Indicates cognitive functioning.Note articulation of speech, including style and content.
Observe the patient’s ability to see, hear, smell, and distinguish tactile sensations.
Rationale: Aids diagnosis and treatment.Observe facial expressions and mood.
Observe movement. (Refer to detailed weight and height measurement procedure.)
Height
Request the patient to remove shoes and stand straight with heels and back touching the wall. Measure height.
Rationale: Aids diagnosis and treatment.Use a height scale to record height.
Weight
Weigh the patient without shoes and heavy clothing.
Rationale: Ensures accurate measurement for diagnosis and treatment.
Inspect and palpate the skin
Assess skin, hair, nails, and overall integumentary health.
Rationale: Aids diagnosis and treatment.
Examine the skin for appearance, texture, sensation, lesions, growths, or trauma.
Check capillary refill by pressing the nail bed and noting the return of color.
Rationale: Helps rule out anemia.
Head
- Inspect the hair for color, texture, growth, and distribution.
Rationale: Detects abnormalities. - Observe the size, shape, and symmetry of the head.
- Palpate the head for deformities, depressions, or tenderness.
Face
Inspect facial expression, asymmetry, involuntary movements, edema, and masses.
Rationale: To rule out paralysis or facial issues.
Eye
Inspect both eyes for position, alignment, symmetry, and color.
Rationale: Detects abnormalities.
Nose
- Inspect the nose’s anterior and inferior surfaces. Gently press the tip of the nose to examine nostrils.
- Use a penlight to view nasal vestibules. Observe for symmetry, size, flaring, and sensation.
Rationale: Detects abnormalities.
Mouth
Observe lips, mucous membranes, gums, tongue, teeth, and palate for color, moisture, texture, and sensation.
Rationale: Detects abnormalities.
Neck
Inspect and palpate the ears for shape, size, symmetry, and patency using an otoscope.
Rationale: Detects abnormalities.Inspect and palpate lymph nodes using the pads of your index and middle fingers. Assess for location, size, shape, texture, and pain.
Includes: Preauricular, postauricular, occipital, tonsillar, submandibular, submental, superficial and posterior cervical, deep cervical chain, supraclavicular nodes.
Rationale: Helps detect infection or other conditions.Inspect and palpate the jugular vein.
Rationale: To rule out distention of jugular veins.
Inspect the thyroid gland
- Ask the patient to extend the neck and swallow. Observe movement, contour, and symmetry.
Rationale: To detect abnormalities.
Palpate the thyroid gland
- stand on the patient’s right side. Ask them to lean slightly forward and swallow while you feel for the gland.
Rationale: Relaxes the sternomastoid and helps assess for enlargement.
Chest,Lung and heart
Ask the patient to sit on the side of the bed and expose the chest. Observe chest movement and symmetry.
Auscultate the lungs and heart.
Breast and Axilla
Inspect the breasts for appearance, color, symmetry, size, shape, and texture.
Nipple
Inspect the nipples for symmetry, shape, scaling, fissures, ulceration, bleeding, or discharge.
Refer to detailed procedure for breast examination.
Expose the abdomen. Ensure hands and stethoscope are warm.
Rationale: To avoid muscle tension and discomfort.Position the patient supine. Inquire about painful areas and examine these last.
Rationale: Prevents muscle guarding.
Inspect the abdomen
- Observe color, shape, symmetry, and any visible pulsations or bulging.
Rationale: Detects abnormalities such as masses or aneurysms. Auscultate bowel sounds before percussion and palpation.
Use the diaphragm to listen to bowel sounds; if absent, listen for 5 minutes. Use the bell to listen for vascular sounds.
Rationale: Prevents alteration of bowel activity; bruit suggests aneurysm.Percuss the abdomen to assess tone.
Rationale: Identifies gas, fluid, or masses.Perform light palpation – depress about 1cm with a rotary motion, moving clockwise across the abdomen.
Rationale: Detects tenderness or superficial masses.Perform deep palpation – use fingertips or bimanual technique for obese patients.
Palpate for kidneys, liver, spleen, and femoral pulse.
Rationale: Detects enlargement, abnormalities, or masses.Ask the patient to stand. Inspect the neck, shoulders, arms, hands, hips, knees, legs, ankles, and feet. Compare both sides.
Rationale: To detect swelling, deformities, or masses.Palpate each joint for tenderness, swelling, or crepitus.
Ask the patient to move joints to assess range of motion.
Rationale: Assesses joint integrity and function.
Nursing Diagnosis (Problem Identification)
Definition
A nursing diagnosis identifies a patient’s actual or potential health problems that require nursing intervention. It is a statement combining signs and symptoms or situations where nursing help is needed.
Components of a Nursing Diagnosis
A nursing diagnosis has three components joined by the phrases “related to” and “as evidenced by”:
Problem: Statement of the actual or potential health issue.
Etiology: Causes or contributing factors leading to the problem.
Signs and Symptoms: Observable or reported characteristics that define the problem.
Examples of Nursing Diagnoses
Actual diagnosis:
Constipation related to inactivity as evidenced by verbal report of failure to pass stool for 3 days.Another example:
Pain related to migraine headache as evidenced by restlessness, irritability, and unusual posture.
Potential Nursing Diagnosis
Consists of only two components joined by “related to” because signs and symptoms are not yet present.
Example:
Potential for bed sores related to limited mobility.
Important Notes
Nursing diagnosis is different from medical diagnosis.
Medical diagnosis identifies the disease or abnormal body function (e.g., lobar pneumonia).
Nursing diagnosis focuses on the patient’s response to the disease or condition (e.g., chest pain related to pneumonia).
Patients may have multiple nursing diagnoses; prioritize based on urgency and threat to life.
| Problem (Diagnosis) | Related Factors (Etiology) | Defining Characteristics (Evidence) |
|---|---|---|
| Activity intolerance | Restricted movement | Verbal report of fatigue or weakness |
| Ineffective airway clearance | Increased bronchial secretions | Abnormal breath sounds |
| Constipation | Inactivity | No bowel movement for 3 days |
| Potential for skin breakdown | Inactivity | — |
| Impaired physical mobility | Limited mobility | Abnormal heart rate or blood pressure |
| Imbalance oxygen supply/demand | — | Response to activity |
| Pain | — | Verbal report of pain, grimacing, holding abdomen |
| Severe anxiety | — | Emotional distress, discomfort, or dyspnea |
| Problem | Etiology (Related to) | Evidence (As evidenced by) |
|---|---|---|
| Constipation | related to prolonged laxative use | — |
| Severe anxiety | related to threat to physiologic integrity | — |
| Risk for infection | related to possible surgical diagnosis | Evidence as available |
.
Planning
Planning is the determination of a course of action to assist the client towards the goal or optimal wellness. In this stage, the nurse refers to assessment findings and nursing diagnoses to design nursing strategies that will prevent, reduce, or eliminate the client’s health problems.
The formulated nursing diagnosis or diagnoses provide direction to the planning process and help in selecting nursing interventions aimed at achieving the expected patient outcome(s). After choosing the interventions, the nurse writes them in the nursing care plan.
Planning Involves:
Setting Priorities
Setting Goals and Objectives
Choosing Appropriate Nursing Interventions
Writing the Nursing Care Plan
1. Setting Priorities
Identify the patient’s needs and problems and rank them in order of priority, giving immediate attention to life-threatening problems.
2. Setting Goals and Objectives
Goals and objectives describe the expected outcome of nursing care. They must be written in terms of expected patient behavior, not the nursing activity.
For goals to be meaningful, they must:
Indicate the expected change in the patient’s condition after appropriate nursing care.
Indicate how the expected change can be observed.
Indicate when the expected change is likely to be achieved (i.e. target date or time).
Goals should be:
Specific
Measurable
Achievable
Realistic
Time-bound
Observable (in terms of behavior, activity, or physical state)
Each Goal Should Consist of:
Subject – The patient or part of the patient (e.g., limbs, vital signs).
Action Verb – Desired performance by the patient.
Criteria – Standard for judging performance.
Time/Date – When it is expected to be achieved.
Manner/Condition – In which the performance is to be carried out (if applicable).
Examples of Goal Statements:
The patient’s temperature will drop by 2°C within 4 hours.
The patient will drink at least 1000ml in 8 hours.
The patient will verbalize his feelings by the end of the week.
A 10-year-old child weighing 18kgs will gain 250g per week and reach 20kgs within four weeks.
3. Selecting Nursing Actions to Meet the Goals
Once the nurse has identified the patient’s problems and established the goals, the next step is to select nursing actions (interventions) that will help meet those goals.
These Selected Actions Should:
Comply with the doctor’s plan of care.
Reflect the priority level of the identified problems.
Be guided by the nurse’s knowledge of nursing theory.
Consider the individual patient’s needs and condition.
4. Writing the Nursing Prescription
A nursing prescription outlines specific nursing measures used to address the diagnosed problems.
Nursing Prescription Must:
Demonstrate ethical behavior that reflects positively on the nursing profession.
Be consistent with the goals and diagnoses.
Align with institutional guidelines and the doctor’s plan of car
Writing the Nursing Care Plan
Each hospital is encouraged to design its own format for the nursing care plan. However, a suggested care plan format should include the following columns:
| Nursing Diagnosis / Patient Problem | Goals / Objectives / Expected Outcomes | Nursing Interventions / Nursing Orders |
|---|---|---|
| Example: Constipation related to inactivity | The patient will pass stool within 24 hours | Encourage fluids, assist with mobility, monitor bowel movements |
| Example: Pain related to migraine headache | The patient will report reduced pain score from 8 to 3 within 1 hour | Provide prescribed medication, ensure quiet environment, apply cold compress |
Example of a Nursing Care Plan
Situation:
Paul is a 10-year-old boy admitted to the surgical ward 4 days ago after sustaining a greenstick fracture of his right femur, resulting from a bicycle collision with a school friend.
Psycho-social History:
First hospital admission
Brought in by parents and friends
Primary Five student at Kabojja Primary School
Enjoys football and riding his bicycle
Clinical Observations:
Height: 125 cm
Weight: 32 kg
Well nourished and physically well developed
Received all childhood immunizations
Nutrition:
Eating very little since admission
States he is not hungry
Elimination:
No bowel movement for 2 days before the accident
Urine appears concentrated
Mobility:
Reluctant to move due to pain
On continuous skin traction for reduction and immobilization
Investigations:
X-ray: Greenstick fracture of the right femur
Urinalysis: No abnormalities
Doctor’s Prescription:
Continuous skin traction with 2.7 kg weight
Paracetamol 500 mg p.r.n. every 6 hours
Review leg and apply crepe bandage
Identified Nursing Problems:
Pain related to fracture and traction
Immobility related to skin traction
Constipation related to immobility
Self-care deficit related to fracture and traction
| Date | Nursing Diagnosis (Actual/Potential Problem) | Goals of Care (Expected Outcome) | Nursing Orders (Nursing Interventions) | Evaluation (Actual Outcome) | Date Solved |
|---|---|---|---|---|---|
| 1. Pain related to tissue damage | The patient will have minimal pain within 2 hours | 1. Administer prescribed analgesics every 6 hours2. Check tightness of traction bandages3. Provide diversional activities4. Maintain proper body alignment5. Perform cold compress 4-hourly | Pain has decreased.Patient is completely free from pain. | ||
| 2. Immobility related to fracture and traction | Patient will regain functional mobility within 8 weeks | 1. Monitor temperature2. Reposition every 2 hours and provide massage3. Massage back, buttocks, and heels4. Encourage active exercises of non-affected limbs5. Teach use of trapeze bar | Temperature is normal.Patient performs exercises willingly and uses trapeze. | ||
| 3. Constipation related to immobility and low intake | Patient will have normal bowel movement within 3 days and maintain regular pattern post-discharge | 1. Encourage high-roughage foods and 2000ml fluid intake/day2. Monitor intake/output3. Offer warm liquids for breakfast (e.g., uji)4. Encourage bowel habits without resistance | Patient ate pawpaw and cabbage.Drank 2500ml/24hrs.Had bowel movement on day 3. | 9/3/2015 | |
| 4. Self-care deficit related to fracture and traction | Patient will increase participation in personal hygiene activities | 1. Place hygiene supplies within reach2. Assist with bathing only for areas he cannot reach3. Encourage independence in self-care | Patient fully participates in personal hygiene. |
IMPLEMENTATION
This is the actual giving of nursing care in accordance with the plan. It is the action phase of the nursing process. Since the term nursing actions involves carrying out doctor’s prescriptions and nursing prescriptions. At all stages of the nursing process, the patient and his/her relatives must be involved as much as possible.
The nurse’s role in assisting patients includes:
Doing for the patient those activities which the patient is unable to do for himself.
Guide the patient carefully on those activities which he can do himself.
Compensate for some need by providing mental and physical support.
Teach and create a therapeutic environment.
Two important steps are involved in implementation:
Determining specific nursing actions that will assist the patient to progress towards expected outcome.
Documentation of care administered.
You won’t be there 24 hours a day and other nurses need to know how the patient is doing and how the plan is working. Nursing actions include both Independent and Collaborative activities.
Independent actions These are activities the nurse performs using his/her own judgment and that require no validation or guidelines from any other health care practitioner.
Collaborative activities These are activities involving decision making, between two or more health care practitioners.
EVALUATION OF NURSING CARE
Evaluation is defined as the fifth and final phase of the nursing process.
It is an on-going process involving the patient, nurse, and other health care team members.
Evaluation refers to measuring the effectiveness of nursing care given in relation to stated goals and objectives.
During this phase, the patient is monitored and data is collected to determine whether progress is being made towards the achievement of the expected patient outcomes.
It also aims to determine whether the patient’s condition has improved.
Evaluation helps to identify:
Goals of care which have been met, as shown by the improvement in the patient’s condition.
If goals are met, the nurse should note and delete them in the care plan.
Goals of care which are being met progressively.
When the patient’s condition progresses favorably, the nursing measures are continued as shown by signs of improvement.
Goals of care which are not met, as shown by no signs of improvement in the patient’s condition, or if the condition is deteriorating.
In this case, the following aspects should be checked:
Was the data collected accurate?
Was the nursing diagnosis correct?
Were the nursing orders appropriate and based on scientific rationale?
Were the nursing measures performed skillfully?
Is there a need to consult other health professionals?
Related Topics
- Wound dressing
- Colostomy Care
- Abdominal Paracentesis(Abdominal Tapping)
- Vulva Toilet/ Swabbing
- Oxygen Administration
- Lumbar Puncture
- Nasogastric tube to feed patients
- Gastrostomy Feeding
- Gastric Lavage
- Catheterization
- Tracheostomy Care
- Caring for patients in traction
- Prepare for application of orthopaedic splints
- Bandaging
- Nursing Process
- Take History of the patient
- Perform a physical examination of the Patient
- Making a Nursing Care Plan
- Admission of a patient
- Drug administration
- Transfer Patients
- Discharge of patients
- Last Office
We are a supportive platform dedicated to empowering student nurses and midwives through quality educational resources, career guidance, and a vibrant community. Join us to connect, learn, and grow in your healthcare journey
Quick Links
Our Courses
Legal / Policies
Get in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2026 Nurses online discussion. All Rights Reserved