Anatomy & Physiology 1
Subtopic:
Muscular System
Learning Objectives
Understand the types of muscle tissue: skeletal, cardiac, and smooth.
Describe the functions of muscle tissue: motion, posture, thermogenesis, and regulation of body cavities.
Explain the physiological characteristics of muscle: excitability, contractility, extensibility, and elasticity.
Understand the structure and organization of skeletal muscle, including connective tissue layers and muscle fibers.
Describe the process of muscle contraction and relaxation, including the role of calcium ions, ATP, and neuromuscular junctions.
Identify major muscles of the face, neck, shoulder, upper limb, back, abdomen, pelvis, hip, and lower limb.
Explain the functions and attachments (origin and insertion) of key muscles.
Understand the role of muscles in movement, posture, and stabilization of joints.
- The term muscle tissue refers to all the contractile tissues of the body.
- These include:- Skeletal/voluntary
- Cardiac (heart)
- Smooth muscle (lymph vessels, stomach, blood vessels, uterus.
- The muscular system how ever refers to the skeletal muscle system.
FUNCTION OF THE MUSCLE TISSUE
Motion
- It is obvious in movements such as walking, running and localized movements such as grasping a pencil or nodding the head.
- These movements rely on the intergrated functioning of bones, joints and skeletal muscles.
- Stabilizing body positions and regulating body cavities in the body
- Besides producing movements skeletal muscle contraction maintain the body in stable position such as standing or sitting.
- In addition the volumes of body cavities are regulation through the contraction of skeletal muscles eg muscles of respiration regulate the volume of the thoracic cavity during eh process of breathing.
- Thernogenesis (heat generation). Regulate body temperature
- As skeletal muscles contract to perform walk and a bi- product of heat is produced.
- Much of the heat released by the muscle is used to maintain normal body temperature.
- Muscle contraction are sought to generate 86% of all body heat.
PYSIOLOGICAL CHARACTERISTICS OF MUSCLES
Muscle tissue has four principle characteristics that enable it to carry out its functions and thus contribute to homeostasis.
Excitability
A property of both muscles and nerve cell. It is ability to respond to certain stimuli.
Contractibility
The ability of the muscle tissue to shorten and contract (shorten) and relax (length) thus generating force to do work.
Sensabiltiy/Extensability
This means the muscle can be extended (stretched) without damaging the tissue
Elasticity
This means that the muscle is able to return to its original shape after contraction or extension eg penis, return.
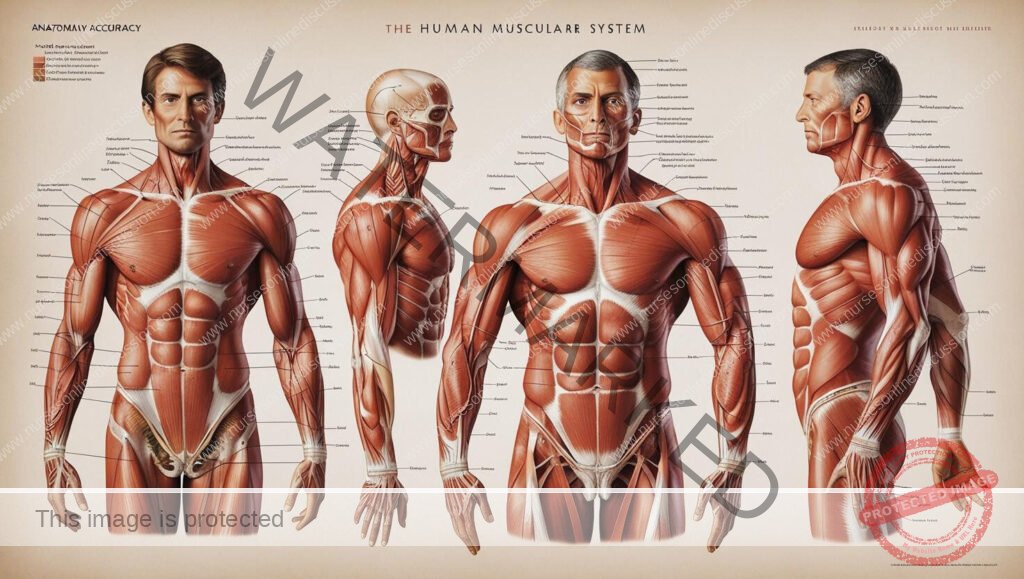
MUSCLE STRUCTURE
A skeletal muscle is an organ composed mainly of striated muscle cells and connective tissue.
Each skeletal muscle has two parts
The connective tissue sheath that extends to form specialized structures that aid in attaching muscle to bone.
The fleshy part ( belly)
- The extended specialized structure maintake the form of a code called a tendon.
- Alternatively abroad sheet aponeourosis which attaches muscles to bones or other muscles. Eg muscle of the skull; Occipito- frontalis muscle. (Helps to raise the eyeballs)
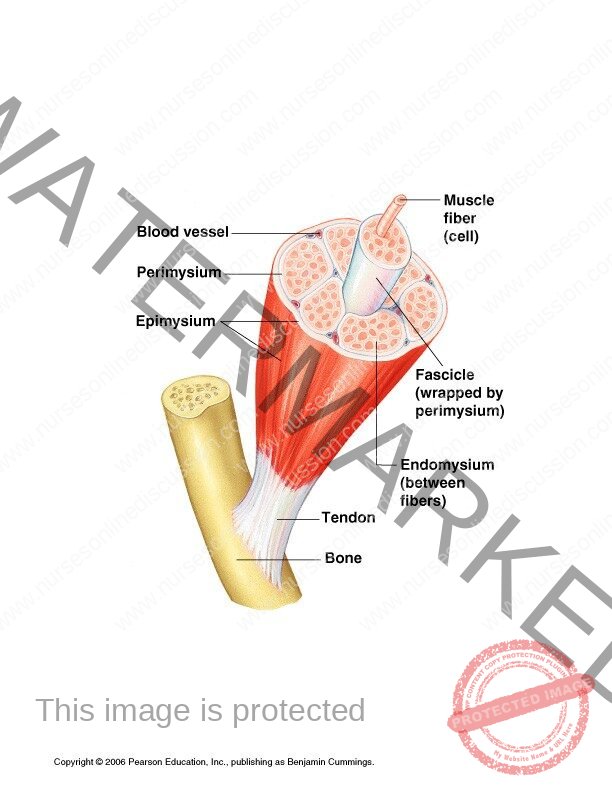
- Connective tissue also extends into the muscle and divides it into numerous bundles. They are three connective tissue components that cover a skeletal muscle tissue these are:-
Epimysium- perimysium- Endomysium
Epimysium
It is a connective tissue that surrounds and separates muscles.
Perimysium
Connective tissue that sorounds each muscle fibre.
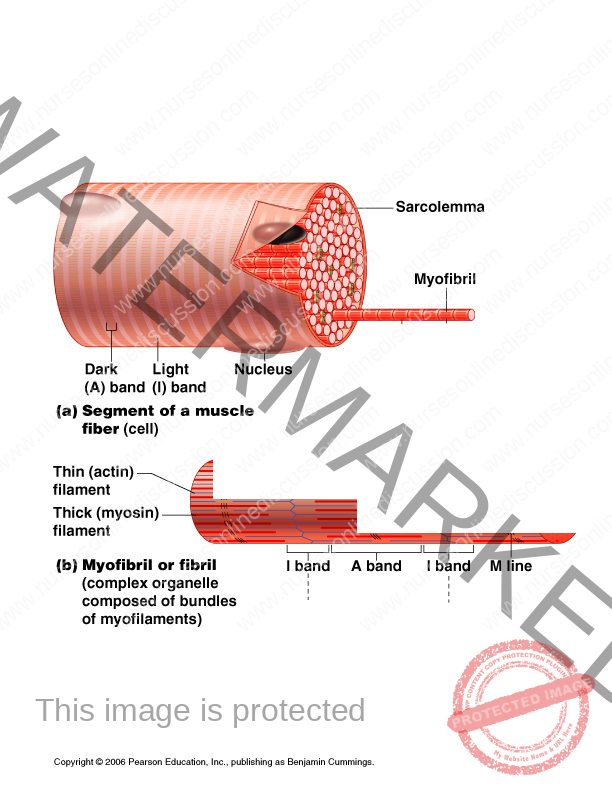
- The muscle bundles are made of very many elongated musclecells called muscle fibres. Each muscle fibre is a cyclindrical cell containing several nuclei located immediately beneath the cell membrane (sacolemma).
- The cytoplasm of each muscle fibre (sarcoplasm) is filled with myofibrils. Each myofibril is a thread like structure that extends from one end of the muscle to the other.
- Myofibrils consist of two major kinds of protein fibres; Actins or thin myofilaments
Myosin or thick myofilament
- There are may mitochondria essential for producing ATP. (Adenosine triphosphate) from glucose and oxygen to power the contractile mechanism.
- Present also is a specialized oxygen- binding substance called myoglobin similar to haemoglobin of Red Blood cells and
- This myoglobin stores oxygen within the muscle.
- In addition, there is extensive intracellular stores of calcium which are released into the sarcoplasm by Nervous stimulation
PROCESS OF CONTRACTION
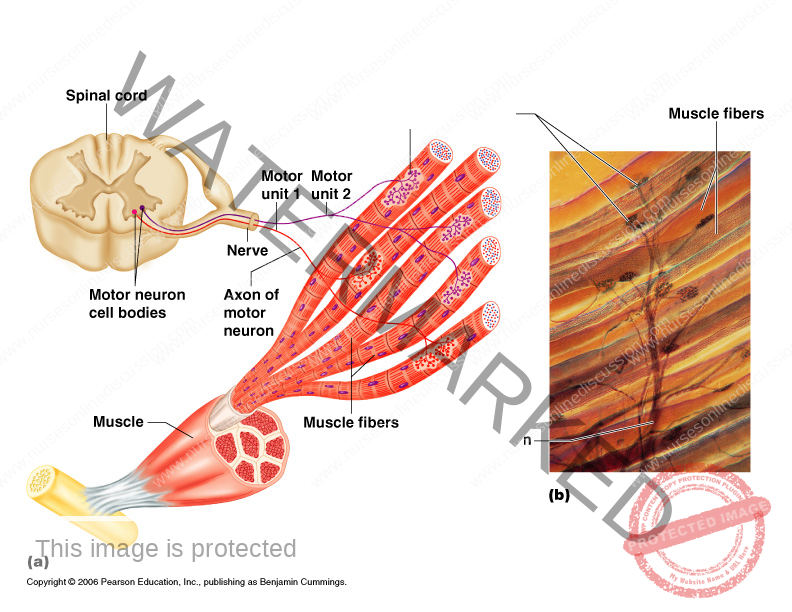
Skeletal muscles contracts in response in stimulation by a nerve fibre which supplies the muscle fibre.
NB: The name given to a synopse between Motor nerve and skeletal muscle fibre is called neuromascular junction.
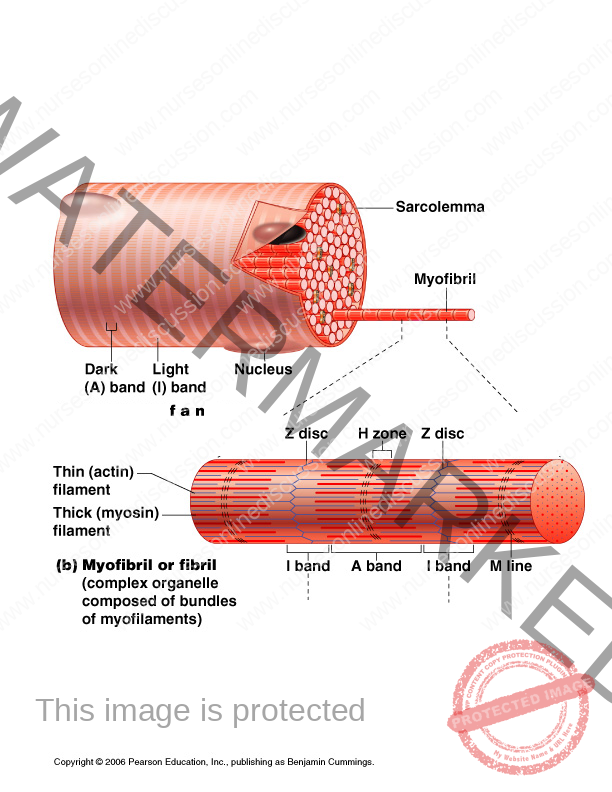
- When a muscle cell is strimulated by a nerve fibre calcium ions are released from intracellular stores, calcium ions triggers the binding of mysin to Action filament next to it forming so called cross bridges.
- ATP then provides energy for the two filaments slide over each other pulling the z- lines at each end of the sarcomere close to one another shortening the sarcomere.
- Muscle relaxes when nerve impulse stimulation stops calcium ions are pumped back into the intracellular stores which breaks the cross bridges between Actin and Myosin filaments. Then they side into their exiginal positions lengthening the sarcomeres and returning the muscle to its original length.
Muscetone
Is a sustained partial muscle contraction that allows posture to be maintained with out fatiguing the muscles involved. Eg keeping the head upright requires constant activity of the muscles of the neck and shoulder.
Muscle fatigue
This results from inadequate oxygen supply as in strainous exercise. It occurs when lactic acid accumulates in working muscles. Fatigue may also occur because energy stores are exhausted or due to physical injury to muscles which may occur after prolonged episode of stranous activity as marathon running.
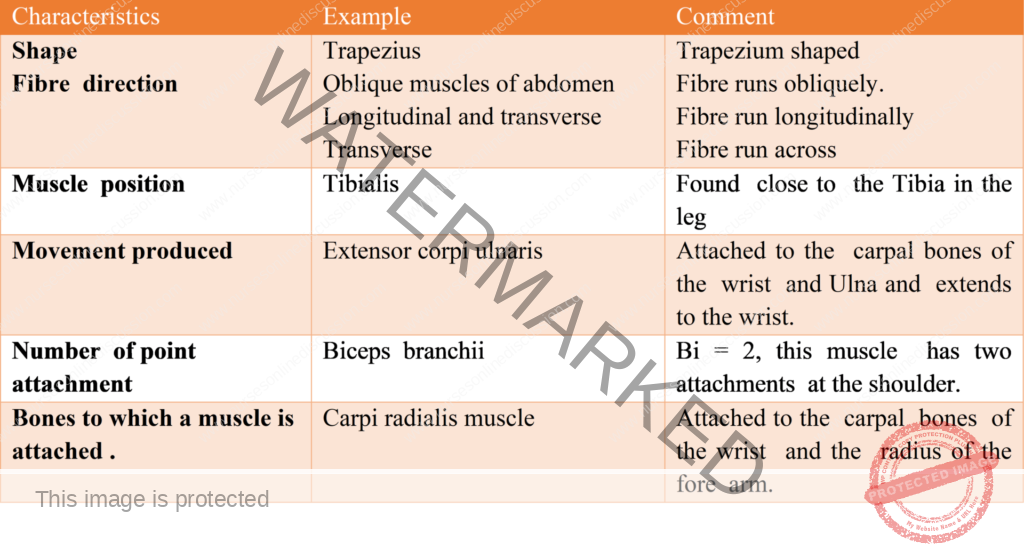
MUSCLE ATTACHMENT
- Most muscles extend from one bone to another and across atleast one movable joint. Muscle contraction causes most body movements by pulling one of the bones towards the other across the movable joints.
- Some muscles are not attached to bones at both ends eg:- some facial muscles attach to the skin which move as the muscle contract.
- The points of attachment of each muscle is it origin and insertion.
- At these attachment points, the muscle is connected to the bone byatendon. The origin is the most stationary end of the muscle and the insertion is the end of the muscle attached to the bone under going the greatest movement.
- Some muscles have more than one origin but the principle is the same. The origin act to anchor/hold the muscle so that the force of contraction cuases the insertion to move.
- Eg the biceps branchi cuases the radius to move resulting in flexion of the forearm.
- The triceps bronchii muscle has three origins ie Two on the humerous and oen on the scapula.
- The insertion of the triceps branchi is on the ulna and contraction results in extension of the fore arm.
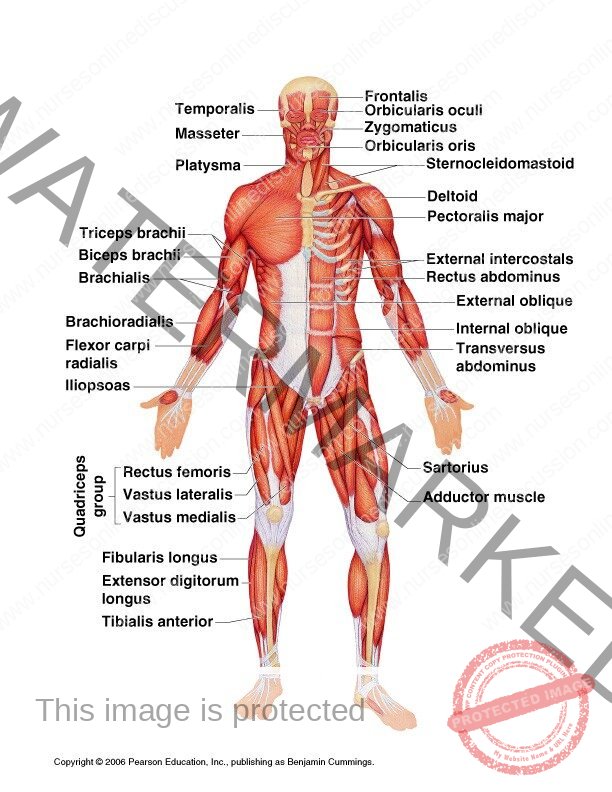
MUSCLES OF THE FACE AND THE NECK
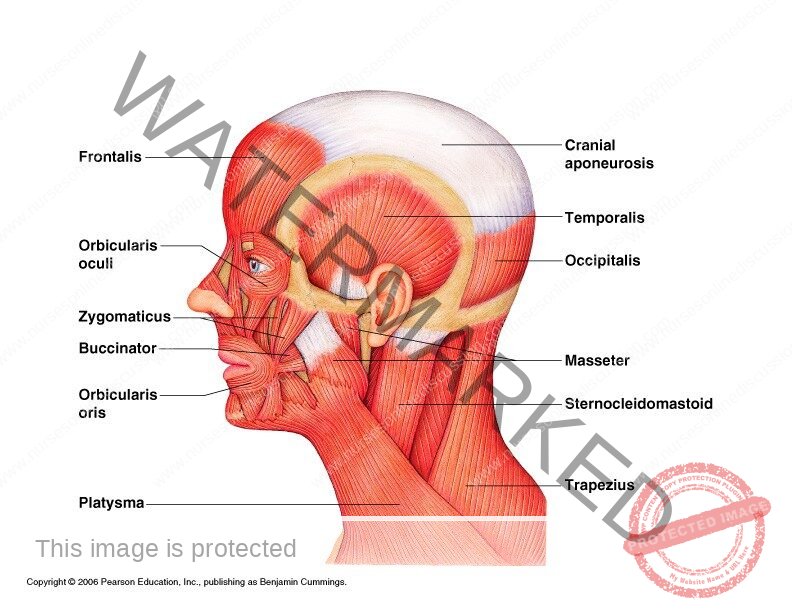
These are involved in changing facial expression, movement of lower jaw during eating and speaking.
MUSCLES OF THE FACE
Occipito- frontalis muscle
This consists of a posterior part which covers the occipital bone (occipitalis). It has an anterior part over the frontal bone (frontalis). It has an extensive tendon or aponuerosis that stretches over the dome of the skull and joins the two muscular parts.
Function
It raises the eye blows.
NB: Write short notes on the following muscles: masseter, buccinators, orbicularis oris, orbicularis oculi, lavatory palpabrae,
MUSCLES OF THE NECK
Sternocleido mastoid muscle
- This rises from the manuarium of the sternum and clavicle and extends upwards to the mastoid process of the temporal bone.
- It insists in turning the head side to side.
- When the muscle on one side contracts it draws the head towards the shoulder.
- When both contract at the same time they flex the cervical vertebra or draw the stemum and clavicle upwards when a head is maintained in a fixed position most especially in forced respiration.
Trapezius
- This covers the shoulders and part of the neck .
- The upper attachment is to the occipital protuberance and the media attachment is transverse process of thoracic and cervical vertebra.
- The lateral attachment is to the clavicle and to the spinous and to the spinous and acromion process of the scapular function.
- It pulls the head back words, and squares the shoulder and control the movement of the scapula when the shoulder joints is in use.
MUSCLES OF THE SHOULDER & UPPER LIMB
These muscles stabilize the association between the appendicular and axial skeleton at the pectral girdle. It stabilizes and allows movement of the upper arm.
Deltoid muscle
- Muscle fibres orginate from the clavicle, acromion process and spine of the scapula and radiates over the shoulder joint.
- It is inserted into the Deltiod tuberosity of the humerous.
- It forms the fleshy and rounded contour of the shoulder.
Function
Helps in the movement of the arm ie flexion, abduction, and rotation of the shoulder joint.
Pectaralis major
- Lies in the anterior from the middle side of the clavicle and sternum and it is inserted into the intertubercular groove of the humenous.
- It draws the arm forward and towards the body ie flexes and adducts.
Caraco branchialis
It lies in the upper medial aspect of the arm. It rises from the coracoid process of the scapula stretches across infront of the shoulder joint. It is inserted into the mid of the humerous.
Function
Flexes the shoulder joint.
Biceps
- Lies on the anterior aspects of the upper arm.
- Its proximal end is divided into two parts (heads) each of which has its own tendon.
- The short head raises from the coracoids process of the scapula and passes infront of the shoulder joint to the arm.
- The long head originate from the rim of the glenoid cavity and its tendon passes through the joint cavity and the bicipital groove of the humerous of the arm.
- Its retained in the Bicipital groove by a transverse humeral ligament that stretches across the groove. The distal tendon cross the elbow joint and is inserted into the radial tuberosity.
- It helps to stabilize as flex the shoulder joint and at the elbow joint it assist with flexion and supination.
Bronchialis
- Lies on the anterior aspect of the upper arm deep to the biceps.
- Originates from the shaft of the humenous, extends across the elbow joint and is inserted into the Ulna just distal to the joint capsule. It is the main flexor of the elbow joint.
Triceps
- This lies on the posterior aspect of the humerous.
- It arises from three heads. One on the scapula and two from the posterior surface of the humerous.
- The insertion is by a common tendon to the acranon process of the Ulna.
- It helps to stabilize the shoulder joint, assists in adduction of the arm and extends the elbow joint.
Branchioradialis
- This spans the elbow joint, originates on the distal end of the humerous and inserts on the lateral epicodyle of the radius. contraction flexes the elbow joint.
Pronator quadratus
- This square shaped muscle is the main muscle causing pronation of the hand and has attachments on the lower sections of both the radius and Ulna.
Pronator teres
- It lies obliquely across the upper king of the front of the fore arm.
- It arises from the medial epicondyle of the humerus and the coronoid process of the Ulna and passes obliquely across the fore arm to be inserted into the lateral surface of the shaft of the radius. It rotates the radioulnar joints, changing the hand from the anatomical to the writing position ie pronation.
Supinator
- Lies obliquely across the posterior and lateral aspects of the fore arm
- Its fibres arise from the lateral epicandyle of the humerus and the upper part of the Ulna and are inserted into the lateral surface of the upper third of the radius.
- It rotates the radioulnar joints often with help from the biceps, changing the hand from the writing to the anatomical position ie supination.
- It lies deep to the muscles.
Flexor carpi radialis
- It lies on the anterior surface of the forearm.
- It originates from the medial epicondyle of the humeos and is inserted into the second and third metacarpal bones.
- It flexes the wrist joint, and when acting with the extensor carpi radials , abducts the joint.
Flexer carpi ulnaris
- It lies on the medial aspect of the forearm.
- It originates from the medial epicondlye of the humerous and the upper parts of the Ulna and is inserted into the pisform, the hamate and the fifth metacarpal bones.
- It flexes the wrist and when acting with the extensor carpi ulnaris, adducts the joint.
Extensor carpi radialis longus and brevis
- These lie on the posterior aspect of the fore arm.
- The fibres originate from the lateral epicondyle of the humerus and are inserted by along tendon into the second and third metacarpal bones. They extend and abduct the wrist.
Extensor carpi ulnaris
- It lies on the posterior surface of the fore arm.
- It originates from the lateral epicandyle of the humerus and is inserted into the fifth metacarpal bone. It extends and adducts the wrist.
Palmaris longus
- This muscle resists shearing forces that might pull the skin and fascia of the palm away from the underlying structures, and flexes the wrist.
- Its origin is on the medial epicandlye of the humerus, and it inserts on tendons of the palm of the hand.
Extensor digitorum
- This muscles originates on the lateral epicondyle of the humerus and spans both the elbow and wrist joints, in the wrist, it divides into four tendons, one for each finger.
- Action of this muscle can extend any of the joints across which it passes ie the elbow, wrist or finger joints.
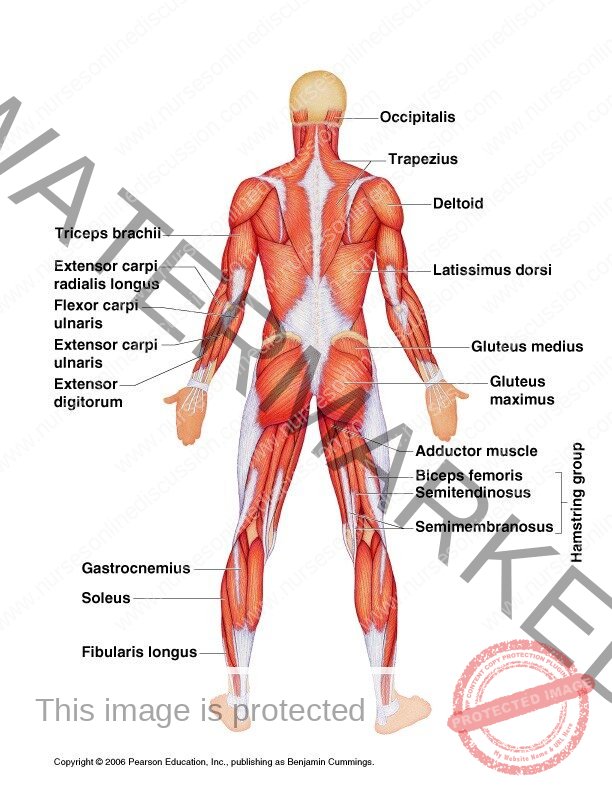
Diagram
MUSCLE OF THE BACK
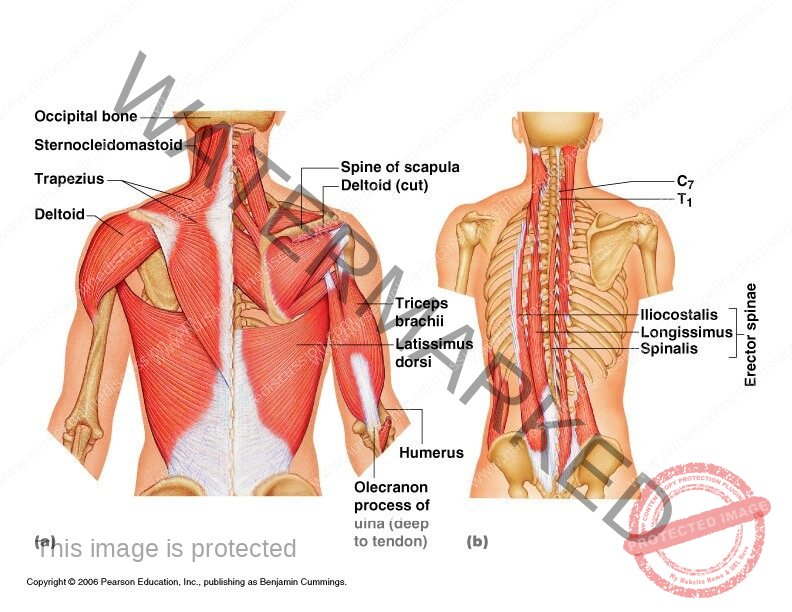
There are six pairs and muscles: Trapezius , Latissimus dosi , Teres major , Psoas ,Quadratas, luborum, Sacro- spinalis
Latissimus dorsi
Arises from the posterior part of the illac crest and spinous process of the lumbar and lower thoracic vertebra. It posses upwards across the back, then under the arm to be inserted into the Biccipital grove of the humerous. It adducts medially rotates and extends the arm.
Quadratas lumborum
Originates from the iliac crest then passes upwards parallel and close to the vertebral column (bending backwards)
If one muscle contracts it causes lateral flexion of the lumbar region of the vertebral column.
Sacro spinalis (Erector spinae)
This is a group of muscles lying between the spinous and transverse processes of the vertebra, originate from the sacrum and is inserted into the occipital bone. Contraction causes extension of the vertebra column.
MUSCLES OF THE ABDOMEN
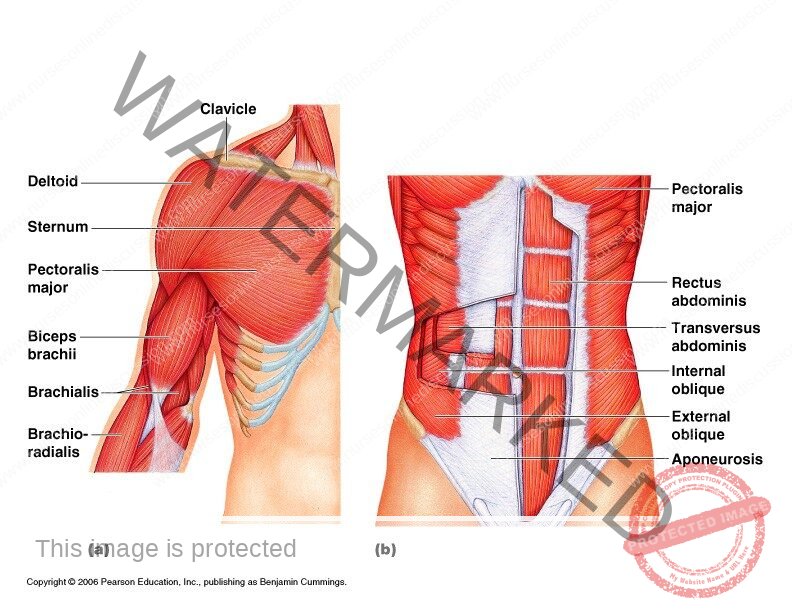
They are five pairs of muscles which form the abdominal wall.
- Eg Rectus abdominis, Internal oblique ,External oblique, Transverse abdominis , Quadrates lumborium
- The anterior abdominal wall is divided longitudinally by a very strong midline of tendinous cord called the linea alba. Meaning the white cord which extends from the xiphoid process on the sternum to the symphysis pubis on the pelvis.
- The structure on each side of the abdominal of the linea alba are identical.
Rectus abdominis
- Is a most superficial muscle. Its broad and flat originating from the transverse part of the pubic bone. It is inserted into the lower ribs and the xiphoid process of the sternum.
- Medially the two muscles are attached to the linea alba.
External oblinque
Extends from the lower ribs downwards and forward. It is inserted into the iliac crest by aponeurosis to the linea alba.
Internal oblique
Lies deep into the external oblique. It is fibres arise from the iliac crest and are inserted into the spinous process of the lumbar vertebra.
It is also inserted into the lower ribs and by an aponeurosis into the linea alba.
Transverse abdominis
- It is the deepest muscle of the abdominal wall.
- It arises from the iliac crest and the lumbar vertebra and passes across the abdominal wall.
- It is inserted into the linea alba by an aponerosis and the fibre are at right angles to those of the rectus abdominis.
Functions
- The main function of those paired muscles is to form the strong muscular anterior wall of the abdominal cavity.
- When these muscles are contracted;
- They compress the abdominal organs.
- They flex the vertebral column in the lumbar region.
- When there is contraction of the muscles on one side, it only bends the trunk towards that side.
- When there is contraction of the oblique muscles on one side it rotates the truck.
MUSCLES OF THE PELVIS FLOOR
- It is divided into two identical halves that unite along the midline.
- Each half consist of fascia and muscles eg Coccygeous
Levator ani
- A pair of broad flat muscles forming the anterior part of the pelvic floor. They originate from the inner surface of the two pelvis and they unite in the midline together they form a sheet that supports the pelvic organs.
Coccygeous
- Paired triangular sheet of muscle, situated behind the levator ani. It originates from the medial surface of the ischium and is inserted into the sacrum and the coccyx. They complete the formation of the pelvic floor which perforated in the males by urethra and anus and females by the anus, urethra, and vagina.
Functions
- Supports organs of the pelvis and resist raised intra pelvic pressure during micturation and defecation.
- The deep muscles of the posterior abdominal wall
MUSCLES OF THE HIP AND LOWER LIMB
Gluteals
- Consist of the gluteus maximus, medius, minimus, minimus, together form the flesh part of the buttocks.
- Originate from the illium and sacrum.
- Inserted into the femur at the linea aspera.
- They cause extension, abduction, and medial rotation at the hip joint.
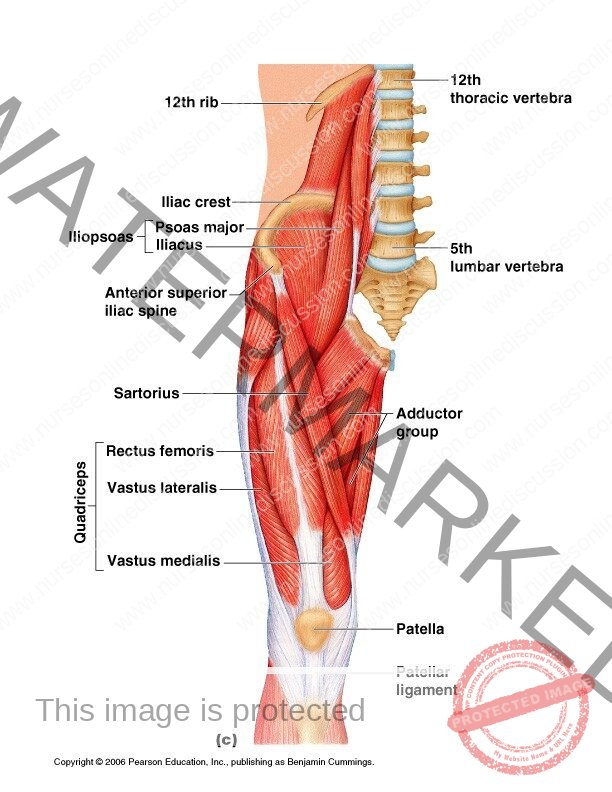
Sartorious
- The longest in the body and crosses both the hip and knee joints.
- Originates from the anterior superior iliac spine.
- Passes obliquely across the hip joint, thigh, and knee joint inserted into the medial surface of the upper part of the tibia.
- Associated with flexion and abduction at the hip joint and knee joint.
Hamstrings
- Lie on the posterior aspect of the thigh
- Originates from the ischium and inserted into the upper end of the tibia.
Function
Flex the knee joint
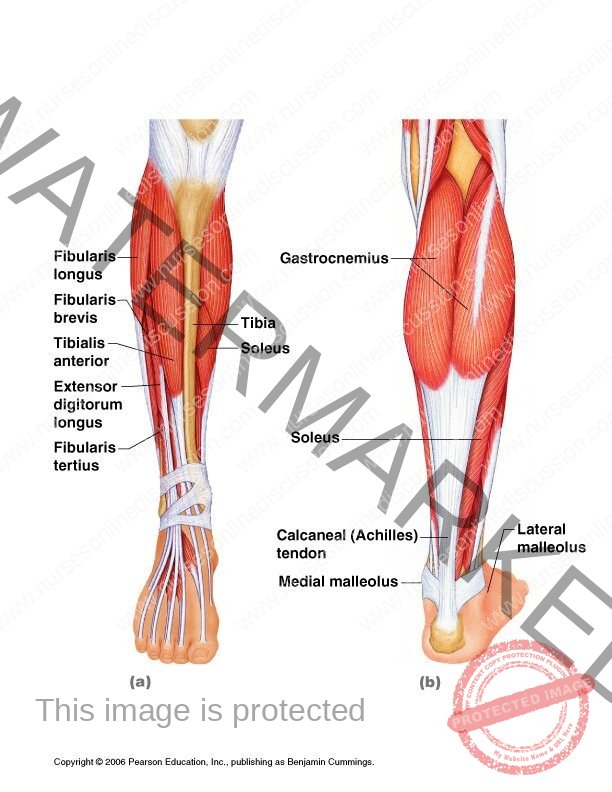
Gastrocremius
- Forms the back of the calf of the leg.
- Arises by 2 heads, one for each condyle of the femur, passes down behind the tibia.
- Inserted into the calcaneous by the calcanean tendon (Achilles tendon)
- It crosses both knee and ankle joints, causing flexion at the knee and plantor (rising into the ball of the foot) at the ankle.
- Others muscles are hip and lower limb: Soleus , Anterior tibialis , Psoas , Quadriceps femoris ,Obturators Abductor group
- Biggest muscles of the body are found here.
- Their function is largely in weight bearing.
- The lower parts of the body are designed to transmit the force of the body weight in walking, running etc, evenly throughout weight- bearing structures and act as shock absorbers.
Psoas
- This rises from the transverse processes and bodies of the lumbar vertebrae. It passes across the flat part of the ilium and behind the inguinal ligament to be inserted into the femur.
- Together with the iliacus it flexes the hip joint.
Iliacus
- This lies on the iliac fossa on the innominate bone.
- It originates from the iliac crest, passes over the iliac fossa and joins the tendon of the psoas muscles to be inserted into the lesser trochanter of the fermur. The combined action of the iliac and psoas flexes the hip joint.
Soleus
- It is one of the main muscles of the calf of the leg, lying immediately deep to the gastrocnemius.
- It originates from the heads and upper parts of the fibia and tibia.
- Its tendon joins that of the gastronemius so that they have a common insertion into the calcaneus by the calcanean ( achelles) tendon. It causes plantar flexion at the ankle and helps to stabilize the joint when standing.
Anterior tibialis
- It originates from the upper end of the tibia, lies on the anterior surface of the leg and is inserted into the middle cuneinform bone by a long tendon. It is associated with dorsiflexion of the foot.
Adductor group
- This lies on the medial aspect of the thigh. They originate from the pubic bone and are inserted into the linea aspera of the thigh of the femur.
- They adduct and medillay rotate the thigh.
Obturators
- These, deep muscles of the buttock, have their origins in the rim at the obturator foramen of the pelvis and in lateral rotation at the hip joint.
Quadriceps femoris
- This is a group of four muscles on the front and sides of the thigh.
- They are the:- rectus femoris, Three vast: lateralis , Medialis ,Intermedius
- The inter medius lies deep in the medialis and lateralis.
- The rectus femoris originates from the ilium and the three vasti from the upper end of the femur. Together they pass over the front of the knee joint to be inserted into the tibia by the patellar tendon.
- Only the rectus femoris flexes the hip joint. Together, the group acts as a very strong extensor of the knee joint.
Join Our WhatsApp Groups!
Are you a nursing or midwifery student looking for a space to connect, ask questions, share notes, and learn from peers?
Join our WhatsApp discussion groups today!
Join NowGet in Touch
(+256) 790 036 252
(+256) 748 324 644
Info@nursesonlinediscussion.com
Kampala ,Uganda
© 2025 Nurses online discussion. All Rights Reserved Design & Developed by Opensigma.co